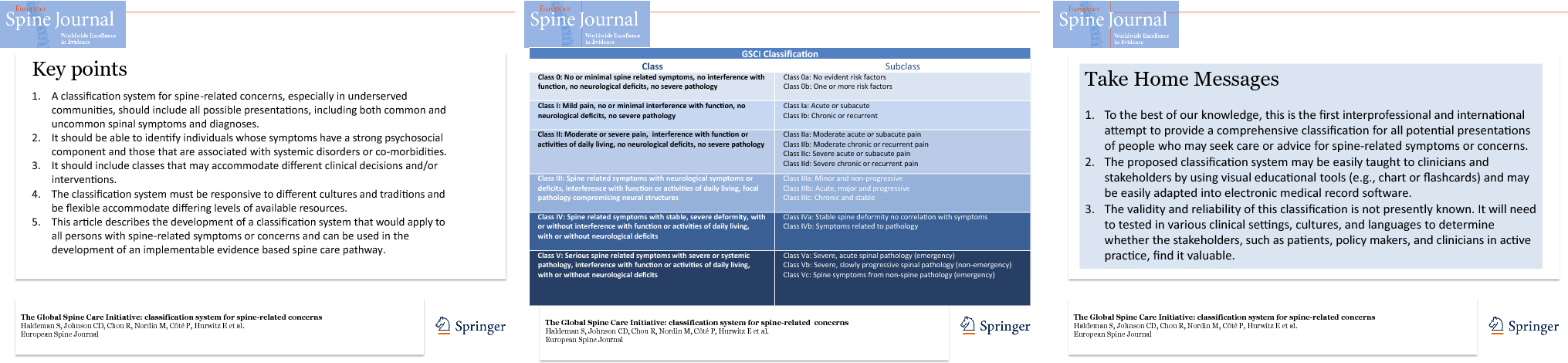
To our knowledge, this is the first interprofessional and international attempt to provide a comprehensive classification that reflects all potential presentations of people who may seek care or advice from a health care provider for spine-related symptoms or concerns. The proposed classification system may be easily taught to clinicians and stakeholders, such as through visual educational tools (e.g., chart or flashcards), and may be easily adapted into electronic medical record software. This classification includes presentations of pain and disability, spine-related neurological symptoms, structural bony pathology, deformities, and serious systemic disease but, at the same time includes people who may benefit from primary or secondary prevention programs. Thus, this classification helps to fulfill the WHO strategies of reorienting models of care [31] to include all people who have or are at risk for specific health problems. This classification also accommodates a person who may present with multiple spine-related concerns. Therefore, a person with multiple concerns may be classified in more than one class (e.g., one class for neck pain and a different class for low back pain). If a patient presents with diffuse non-focal pain, the area would be noted and the classification compatible with its severity, chronicity, and functional interference would be assigned.
This classification was not developed to replace other spinal disorders classification systems. Instead, it incorporates most other attempts at categorizing spinal disorders and, at the same time, addresses all people with spine-related symptoms or concerns. Depending upon the social and environmental situation, level of resources, or clinical setting, any of the classes could be considered, included, or removed. Thus, it can be adapted to different environments in clinical, research, or policy development settings. A clinician or researcher who elects to follow the Quebec Whiplash or Bone and Joint Decade Task Force recommendations may choose to limit their consideration to Classes I, II, III and elect not to include the other classes or subclasses. A clinician or researcher whose primary concern is non-specific low back pain may focus on the NIH Research Standards as noted in Classes I and II and include the subclasses addressing pain severity and chronicity. Surgical considerations would likely focus on patients in Classes III, IV, and V who might reasonably be considered candidates for surgery. A population-based primary prevention program would likely focus on Class 0. A rheumatologist or infectious disease specialist would likely focus on Class V presentations. The comprehensive spine care pathway could reasonably be implemented in communities with limited resources and therefore may incorporate the entire classification system. This classification allows for the determination of which individuals can reasonably be served at different levels of resources.
This spinal classification has language that can be used by any discipline and is simple enough to be easily taught to clinicians or stakeholders irrespective of their training or experience. The classification can differentiate people with spine-related symptoms that would likely require a different clinical decision or intervention pathway. Due to its design, it can match population needs where there are limited resources and therefore avoid over-medicalization of spine pain by avoiding the recommendation for a pathological diagnosis for most people who present with spine pain and disability but no red flags for serious pathology. Furthermore, it also accommodates the small number of people who may present with red flags for neurological deficits or serious pathology that may require emergency, surgical, or advanced pharmaceutical interventions.
The GSCI classification is consistent with most current survey and classifications systems. The classification has been informed by individuals participating in the modified Delphi processes as well as the systematic reviews and other articles being produced as part of the GSCI [1, 2, 3, 4, 5, 6, 24, 25, 26, 27, 28, 29, 32, 34]. It forms the basic framework for the GSCI care pathway and recommendations for implementation of a model of care. The classification is linked to systematic reviews of the scientific literature for public health, assessment, noninvasive as well as invasive interventions so that it may be useful in the clinical setting. The review of the evidence provides the basis for determining the indications and contraindications for each of the multiple interventions that may be considered for people who fall into one or more of these classifications.
The classification is flexible in that it can be used to address the entire spine or can be applied separately to different spine regions or pathological processes. An individual could be classified into one or more class at the same point in time. For example, a person could be in Class I for low back pain and Class II for neck pain. Therefore, a patient with a combination of spinal regions, symptoms, or pathological states may be accommodated in this classification.
This classification is person-centered and can accommodate individuals with spine symptoms that vary over time and have different levels of severity and chronicity. It allows an individual with spine symptoms to be assigned to more than one class; thus, classes are not mutually exclusive. The classification may be applied to a person entering or re-entering the system with symptoms suggestive of the same or a different class of spinal disorder, thus allowing for the realities of practice. At the same time, when matched with intervention guidelines and epidemiologic research it can be used by clinicians to inform their patients about diagnoses, intervention considerations, and prognoses. For the purposes of the GSCI, this document has informed the development of the care pathway and model of care.