September 2019, Volume 28, Issue 9, pp 1889–1905|
Le Huec, J.C., Thompson, W., Mohsinaly, Y. et al. Eur Spine J (2019) 28: 1889. https://doi.org/10.1007/s00586-019-06083-1
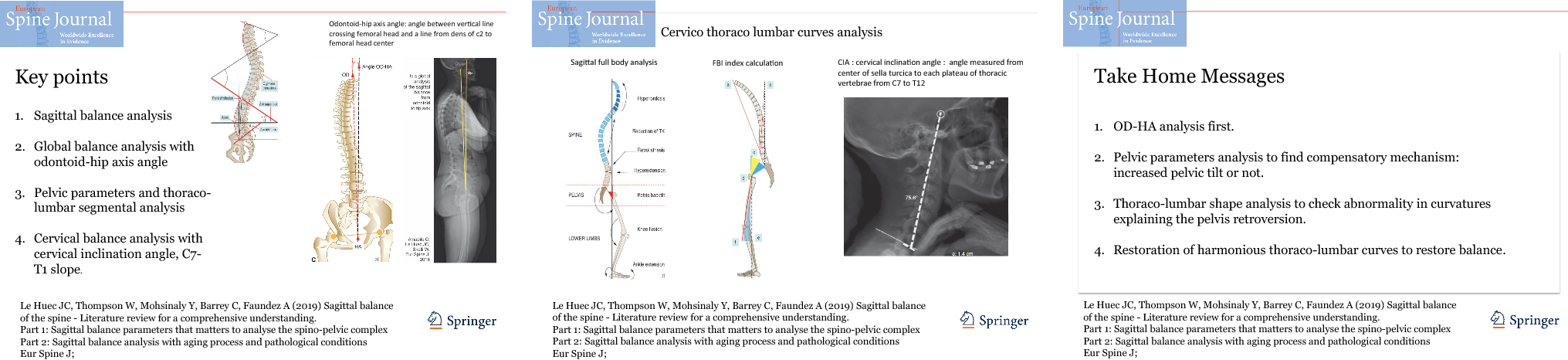
The static sagittal balance of the normal spine is a physiological alignment of the spine in the most efficient manner by the muscular forces. During gait, this balance is constantly thwarted by single-foot support. This analysis involves the study of parameters which are now well defined. The pelvic incidence is constant, and the sacral slope and the pelvic tilt are positional. The cervical parameters are the upper (O–C2) and lower cervical curvatures (C2–C7), the C7 slope, the spino-cranial angle and the vertical cervical offset. At the thoracic and lumbar level, they are, respectively, kyphosis and lordosis. The OD-HA (odontoid hip axis) angle is the most efficient parameter to analyse the global balance. The average values of these parameters are reported with the new 3D measurements by Le Huec et al. The relationship between these different parameters was analysed, and Roussouly proposed his classification of the different spine shape. Ageing makes it possible to show compensation mechanisms at three levels: spinal, pelvic and lower limbs. Understanding these different data allows for better planning of the surgical management of the patients. Global evaluation of the entire spine and the measurement of the aforementioned parameters allow to determine the extent of the correction to be performed during surgery. Taking these parameters into account also enables us to understand the complications involved in this type of surgery: transitional syndromes or junctional syndromes. Integration of these parameters into the study of gait is an area still under investigation.
These slides can be retrieved under Electronic Supplementary Material .
Sagittal balance Spinal balance Spinal imbalance Junctional syndrome Lumbar lordosis Pelvic tilt Global balance analysis Spino-pelvic parameters Spino-cranial angle FBI
The online version of this article ( https://doi.org/10.1007/s00586-019-06083-1) contains supplementary material, which is available to authorized users.
A correction to this article is available online at https://doi.org/10.1007/s00586-019-06128-5.
Balance or equilibrium (from the Latin aequilibrium, from aequus “equal” and libra “balance, weight”) is a concept that describes a situation in which the forces present are equal, or such that none surpasses the sum of the others. It is in this condition that the actions of the agonist and antagonistic muscles of the spine are minimized and therefore most efficient.
The human species is characterized by bipedalism, which has the advantage of freeing the upper limbs for other tasks, but this is done at the cost of a more precarious overall balance. Indeed, the great apes, unlike humans, move on all the four. Their spine presents a single thoraco-lumbar curvature in kyphosis. Their centre of mass is projected at the centre of their support polygon which is located in front of the footprint of the hind legs.
The hominids modified their profile by developing cervical curvature and lumbar lordosis to maintain a horizontal gaze and to free the upper limbs that are no longer carriers. To understand the conditions necessary for such a balance, it is important to analyse matters both statically and dynamically.
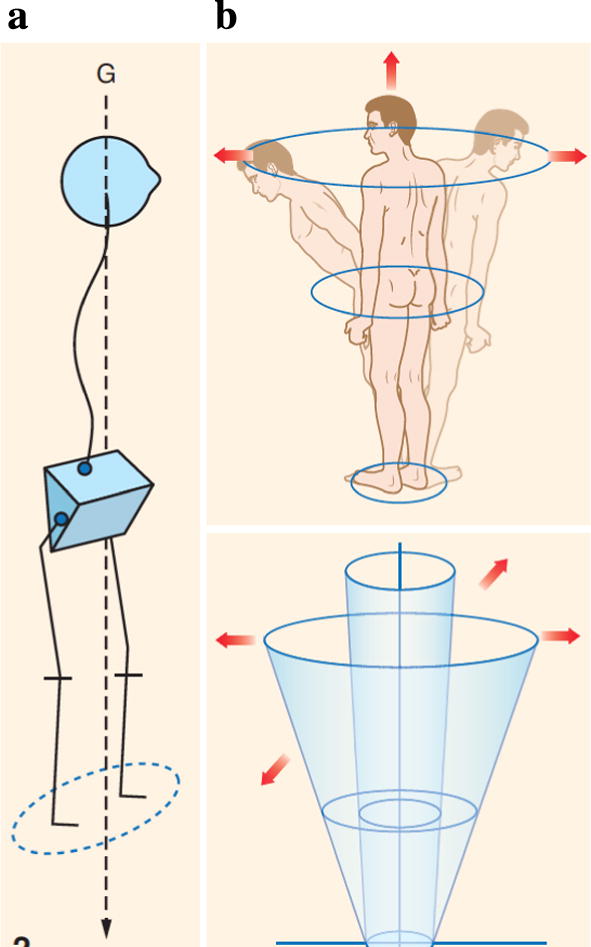
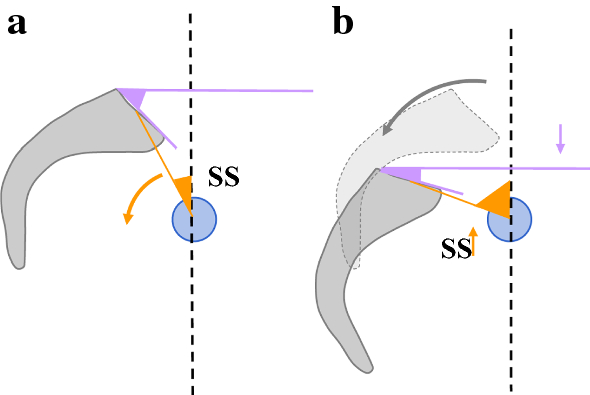
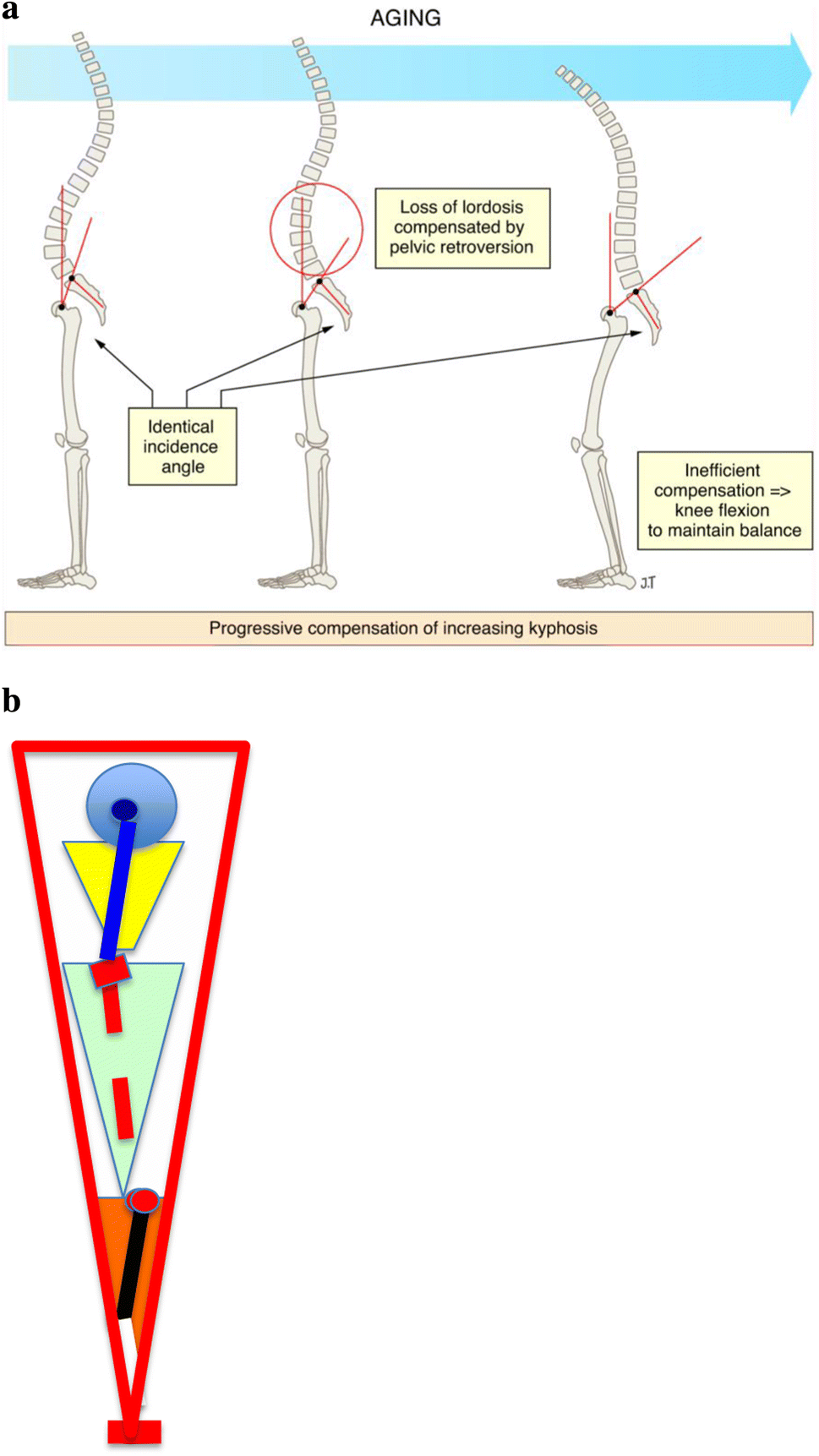
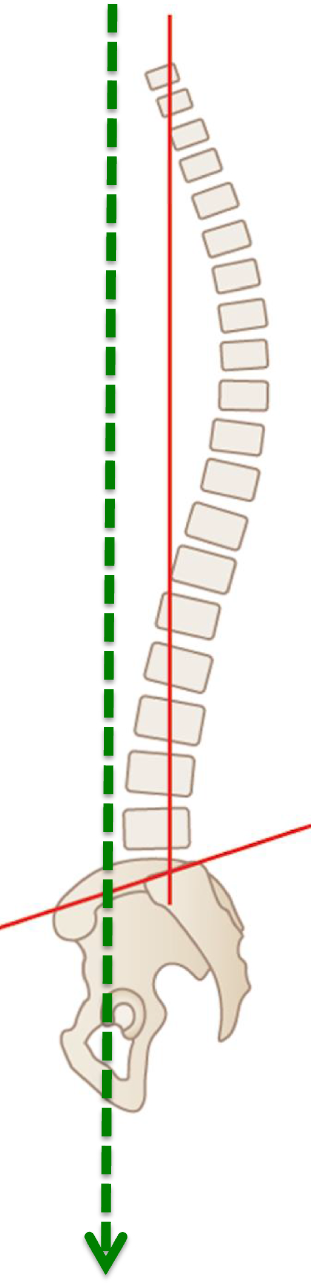
Indeed, during gait, bipedal static balance is constantly thwarted by single-foot support while stepping and must be compensated by a muscular tolerance which tends to reestablish this balance by passing through short phases of instability. As will be seen, sagittal balance is not limited to the analysis of static curves, as it requires consideration of more or less efficient compensation phenomena occurring during walking but also in static conditions.The centre of mass should project as close as possible towards the centre of a reduced polygon situated between the two feet in a stable position and in an area of constant small rebalancing efforts. If the centre of mass tends to project outside this polygon, the rebalancing efforts become much more important, as described by Dubousset in his concept of “efficiency cone” (Fig. 1a, b) [1].
The purpose of this chapter is to describe the morphologic criteria that can be analysed to determine static sagittal alignment of the spine, and to then analyse the compensation phenomena which may be physiological or pathologic. The chapter also aims to use the parameters and algorithms that allow global analysis to provide therapeutic solutions adapted to each case.
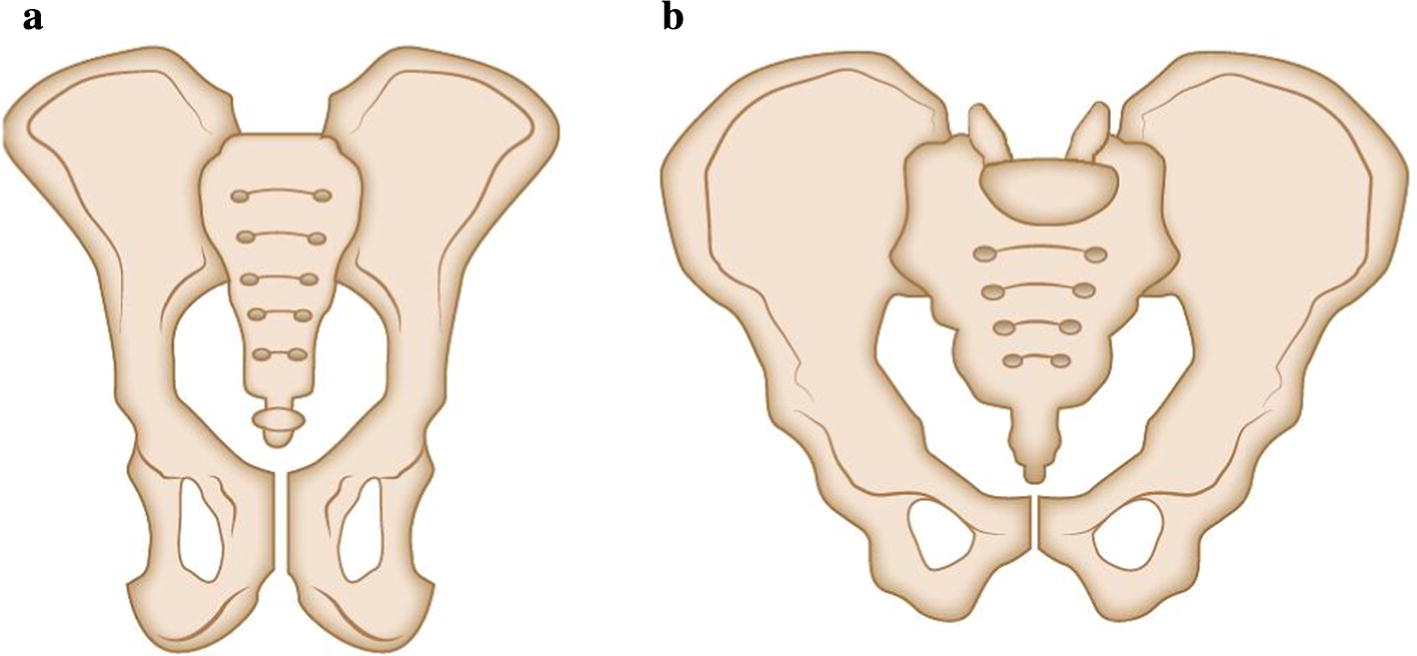
A human being stands and moves in an environment subject to gravity. Its spine is subject to subsequent constraints. There is a close relationship between the pelvis and the spine due to this bipedal position. The upright posture is acquired by the enlargement and verticalization of the pelvis (Fig. 2a, b), leading to the characteristic curvatures of the vertebral column in sagittal plane. Unlike some species, such as chimpanzees, that adopt the erect position only occasionally, the latter is the preferred posture in humans. It must therefore be stable and efficient.
The pelvis must be considered as a “pelvic vertebra” or first vertebra of the spine, as proposed by Dubousset [1]. The location of this base determines the position of the lumbar spine and hence of the entire vertebral column. In the frontal plane, the alignment is simple: The vertebral column is vertical with a median axis that passes through the middle of the sacrum.
The geometries of the pelvis and of the vertebral column in the sagittal plane are more complex. To better understand sagittal alignment, we must examine the position of the centre of gravity and the resultant line of gravity.
These two parameters have been studied by many researchers. The line of gravity is determined from force platforms (a device that represents the vertical projection of the sum of ground reaction forces, of a standing person) [2].
In the sagittal plane, this line of gravity is a line perpendicular to the ground which passes slightly behind the femoral heads in normal well-aligned subjects [2, 3]. In a well-aligned and balanced person, this line of gravity is projected onto the ground and delineated by the feet. The centre of gravity is located on this line in front of the S2 vertebra when the arms are alongside the body. Conventional imaging, such as magnetic resonance imaging (MRI) or computed tomography (CT), is not very useful to analyse balance because patients are lying down. It is therefore important to produce long-standing radiographs. Although the gravity line is an interesting parameter, it is not very usable because imaging devices are rarely coupled to force platforms. It is therefore essential to determine parameters that measure sagittal balance indirectly and therefore detect pathologic conditions by the radiographic analysis of standing persons keeping in mind that roughly the gravity line crosses the femoral heads on a sagittal view [2, 3].
The first pelvic parameter to be considered is pelvic incidence (PI). The pelvic incidence corresponds to the angle between the perpendicular to the upper S1 level passing through its centre and the line connecting this point to the axis of the femoral heads [4] as described by Legaye and Duval-beaupère [5].
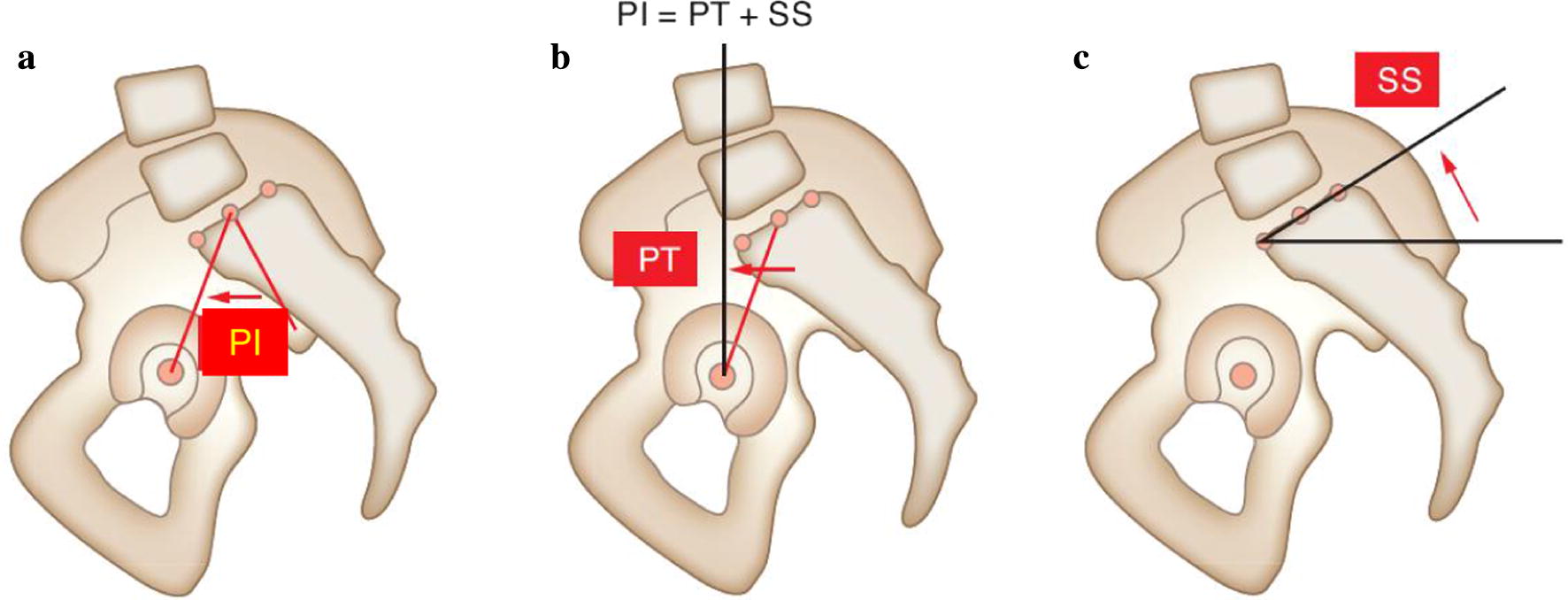
It is an anatomical parameter, constant for each individual, independent of the spatial orientation of the pelvis. In fact, this angle involves the first three sacral vertebrae, the two sacroiliac joints and the posterior margin of the iliac wings up to the acetabulum.
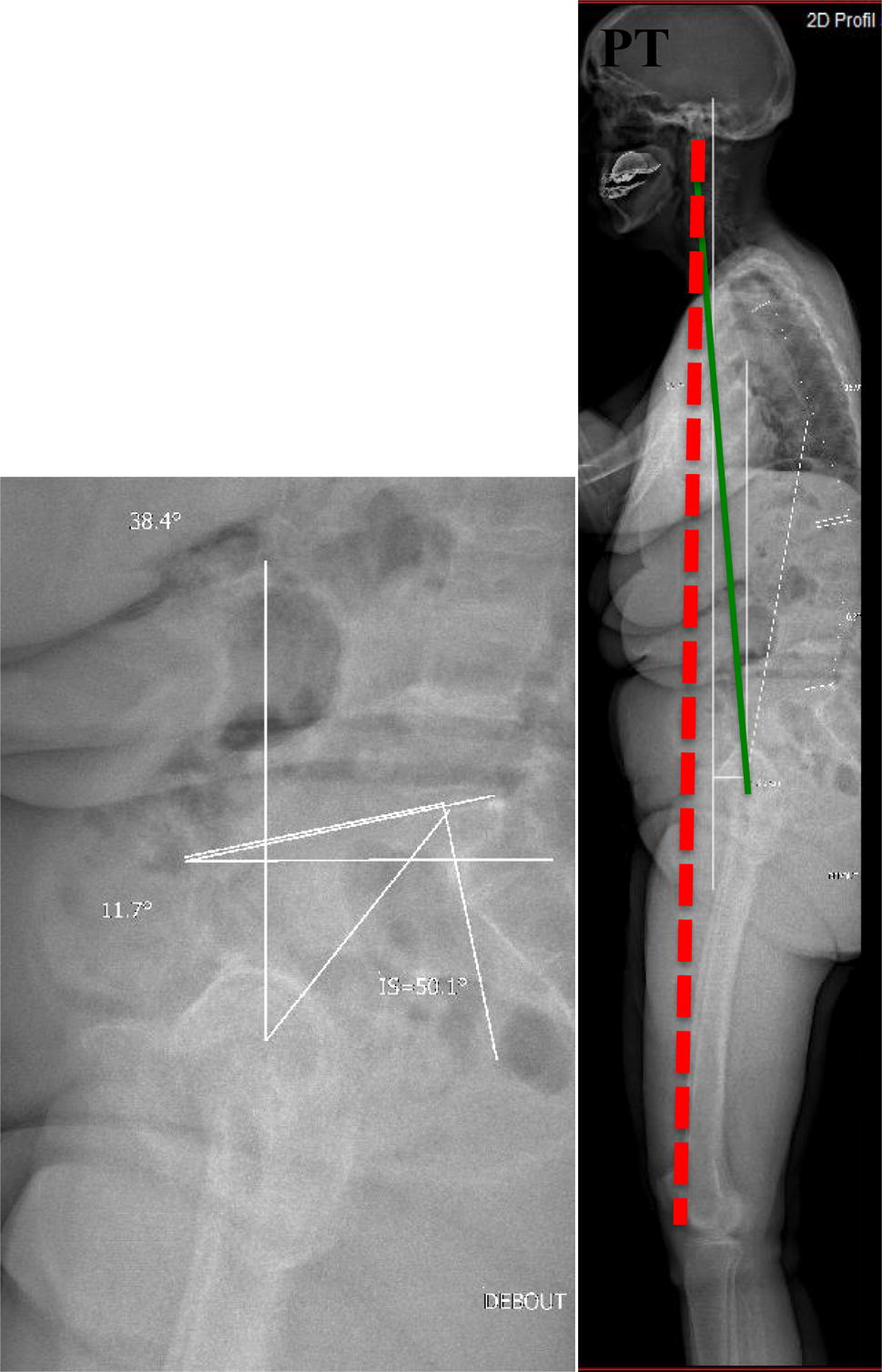
The mobility of the sacroiliac joints is considered negligible beyond childbirth. Thus, once growth is complete, the pelvic incidence remains constant in a given individual. A small pelvic incidence angle corresponds to a narrow pelvis (small anteroposterior dimension), while a large angle indicates a broad one (large anteroposterior dimension). In elderly over 75 years old, or some specific long fusion constructs, ligament loosening can produce some degrees of variations [6, 7, 8].The sacral slope (SS) is defined by the angle between a line tangent to the upper S1 endplate and horizontal line. A vertical pelvis implies a low sacral slope, while a horizontal pelvis would have a high slope. The pelvic tilt (PT) is defined by the angle between the vertical and the line connecting the centre of the sacral endplate to the axis of the femoral heads. Those two angles are positional and related to pelvis orientation. This is possible because the pelvis can rotate around the axis of the femoral heads. This movement can be forwards (anteversion, Fig. 4a) or backwards (retroversion, Fig. 4b). The pelvic tilt (PT) angle increases during retroversion of the pelvis (Fig. 4a, b).
There is a relationship between these three parameters [5] (Fig. 3): The pelvic incidence is equal to the arithmetic sum of the sacral slope and the pelvic tilt (PI = PT + SS). It follows that a patient with a high pelvic incidence angle has a greater potential for pelvic retroversion. This is an important knowledge when analysing the compensatory mechanisms.
To each angle of pelvic incidence, correspond a theoretical value of sacral slope and pelvic tilt in a normal asymptomatic population. Several studies have successfully stratified these values according to the pelvic incidence value [9, 10]. The more recent formula [9] is given by the 3D analysis of the full spine in standing position by: theoretical pelvic tilt = 0.44 PI − 11° in a normal asymptomatic population. Therefore, it is possible to know whether the pelvic tilt measured on a X-ray taken in standing position is normal or abnormal because the pelvic tilt is a positional angle depending on the orientation of the pelvis.
There are three successive curvatures from cranial to caudal: cervical lordosis, thoracic kyphosis and lumbar lordosis [5].Cervical parameters [11] (Fig. 5a): lower cervical shape is measured between the C2 endplate and the lower C7 endplate. The cervical spine may feature some lordosis or kyphosis, or may indeed be neutral, depending on the value of the C7 slope [11]. Cervical shape can be separated into two angles:
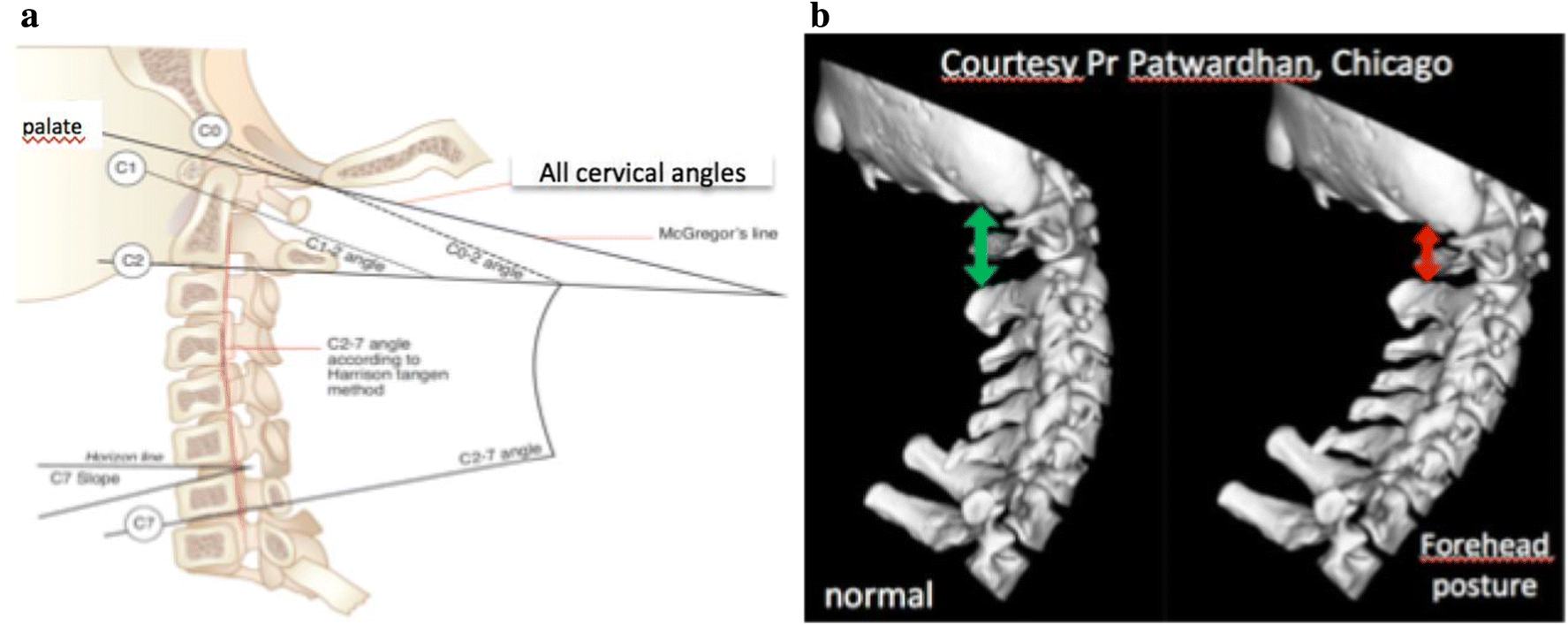
O-C2 and C2–C7 angles work inversely: When one is increasing, the other one is decreasing (Fig. 5b).
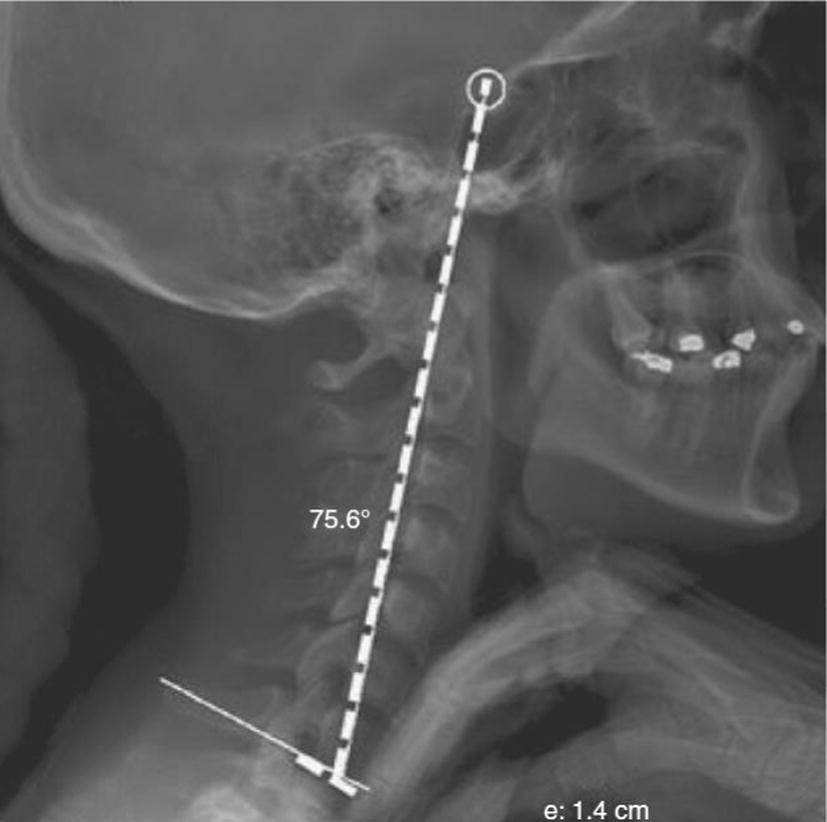
The C7 slope is a key parameter for studying the cervical spine statically [11]. The median value is 20°. Patients with a C7 slope greater than 20° have a lordotic cervical spine (lordosis between C2 and C7). Patients with a C7 slope of less than 20° have a neutral or kyphotic cervical spine between C2 and C7.The spino-cranial angle (SCA) (Fig. 6) corresponds to the angle between the tangent to the upper C7 plateau and the line connecting the middle of the upper C7 plateau to the centre of the sella turcica [11]. In asymptomatic persons, the SCA value is constant with a mean of 83° ± 9°. It is an important angle because it provides an idea of the head offset over C7–T1.
The vertical cervical offset, also called cervical SVA, corresponds to the horizontal distance of the C2 and C7 plumb lines. It is a way to analyse the offset of the head.
Thoracic kyphosis is measured between the upper T1 endplate and the lower T12 endplate. It has been shown that the theoretical value of thoracic kyphosis is equal to 0.75 times the global lumbar lordosis angle, L1 to S1 [9]: T1T12 lordosis = 0.75 × L1S1 lordosis.
However, many articles measure thoracic kyphosis between T4 and T12 because of the poor quality of normal radiographs due to the superposition of the humeral heads. Using EOS imaging technology [12], Le Huec and Hasegawa have recently published the value of T1–T4 kyphosis in an asymptomatic population [9]. This study shows that this segment of the kyphosis represents 8° to 10° of the overall thoracic kyphosis. This fact is essential because many thoraco-lumbar posterior fusion constructs stop at T4 and therefore ignore the residual lever arm of the suprajacent body segment. Analysing the position of the head and its relationship with the thoracic shape with the cervical inclination angle (CIA), it has been demonstrated that the T1T5 segment is the base of support for the cervical spine with the CIA angle (a line from sella turcica to the vertebral plateau of a thoracic vertebra and a line parallel to the chosen vertebral plateau are constant in an asymptomatic population) [13].
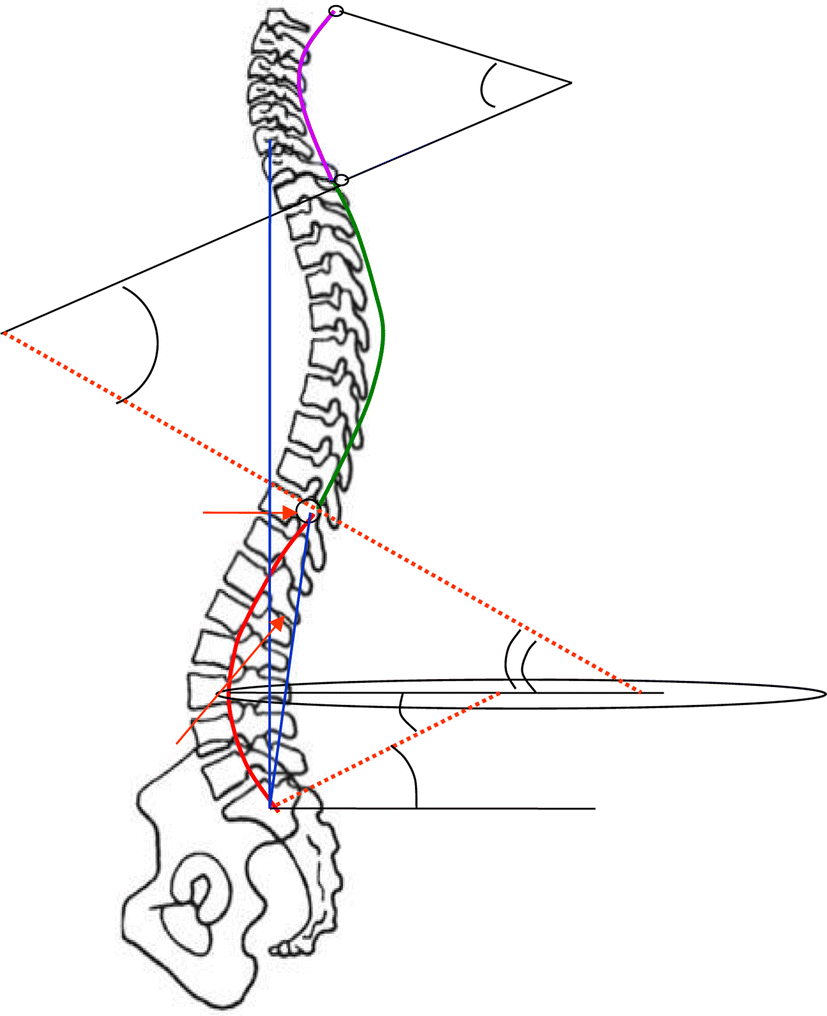
The lumbar lordosis (LL) according to Roussouly is measured between the point of inflection from lumbar lordosis to thoracic kyphosis and the upper S1 endplate (Fig. 7) [14]. This point is geometrically calculated when the lumbar lordosis turns to the thoracic kyphosis. Using this new analysis, it is shown that two-thirds of the lumbar lordosis are located at the last two lumbar levels as previously reported by Jackson [15] and confirmed by Roussouly [16]:L4S1=0.66×L1S1[16]L4S1=0.66×L1S1[16]
A recent retrospective study suggested that this percentage of distal lordosis varies by a few degrees according to the PI value. However, the proximal lordosis seems to be significantly influenced by the PI value (greater PI, more proximal lordosis) [17].
There is a close relationship between lumbar lordosis and pelvic incidence. Berthonnaud proposed a model that divides the lumbar lordosis into two tangential arches (Fig. 7) [18]. The lower arch is constructed by the horizontal line passing through the apex of the lordosis and by a line tangent to the sacral endplate. The upper arch corresponds to the angle measured between the horizontal line passing through the apex of the lordosis and another passing through the point of inflection. The superior arch has a constant value between 15° and 19° [18]. The inferior arch varies depending on the orientation of the sacral endplate and corresponds to the value of the sacral slope. There is a strong correlation between sacral slope and lumbar lordosis (r = 0.86, p < 0.001). The relation between the sacral slope and the pelvic incidence explains the link between pelvic incidence and lumbar lordosis. Several studies sought to find a mathematical relationship between lumbar lordosis and pelvic incidence.
Legaye [4] demonstrated predictive formulas for lumbar lordosis as a function of pelvic parameters and vertebral rotation for scoliotic patients. These are the first predictive formulas for calculating lumbar lordosis. However, this study is limited because of the small number of patients. Schwab [19] proposed the following formula: PI = LL ± 9° which again was calculated on a small number of subjects and therefore has poor accuracy for the low and high values of pelvic incidence leading to errors in daily practice.Recently, Roussouly [10], with a large database using standard full spine and Le Huec [9], combining 3D databases using low-dose EOS imaging technology on 268 healthy adults from various ethnicities (proved by functional and pain scores: VAS, Oswestry, SF36 and SR22), has proposed a new formula for lumbar lordosis (LL):LL(L1−S1)=0.54×PI+27.6LL(L1−S1)=0.54×PI+27.6The value of this formula, calculated from a statistically powerful sample, in 3D and without possible distortion, is therefore more accurate than formulae derived from a statistically weak sample. This study also derives quite simple formulas relating the pelvic incidence to the pelvic tilt and the sacral slope:PT=0.44PI−11.4PT=0.44PI−11.4
Using those formulas allows to know the theoretical normal value of SS and PT for asymptomatic healthy young population when the PI is measured, and detect a compensating pelvic retroversion, for instance, in pathologic cases.In a prospective study of normal asymptomatic subjects, Roussouly [10] considered these different spinal and pelvic parameters to define four types of spines (or spino-pelvic types), in particular taking into account the inflection point (corresponding to the transition biomechanical from “lumbar lordosis” to “thoracic kyphosis”) (Fig. 8). This is the first classification described to stratify the population’s spine shape, which is a continuum, to categories to help to understand the spine pathologies.
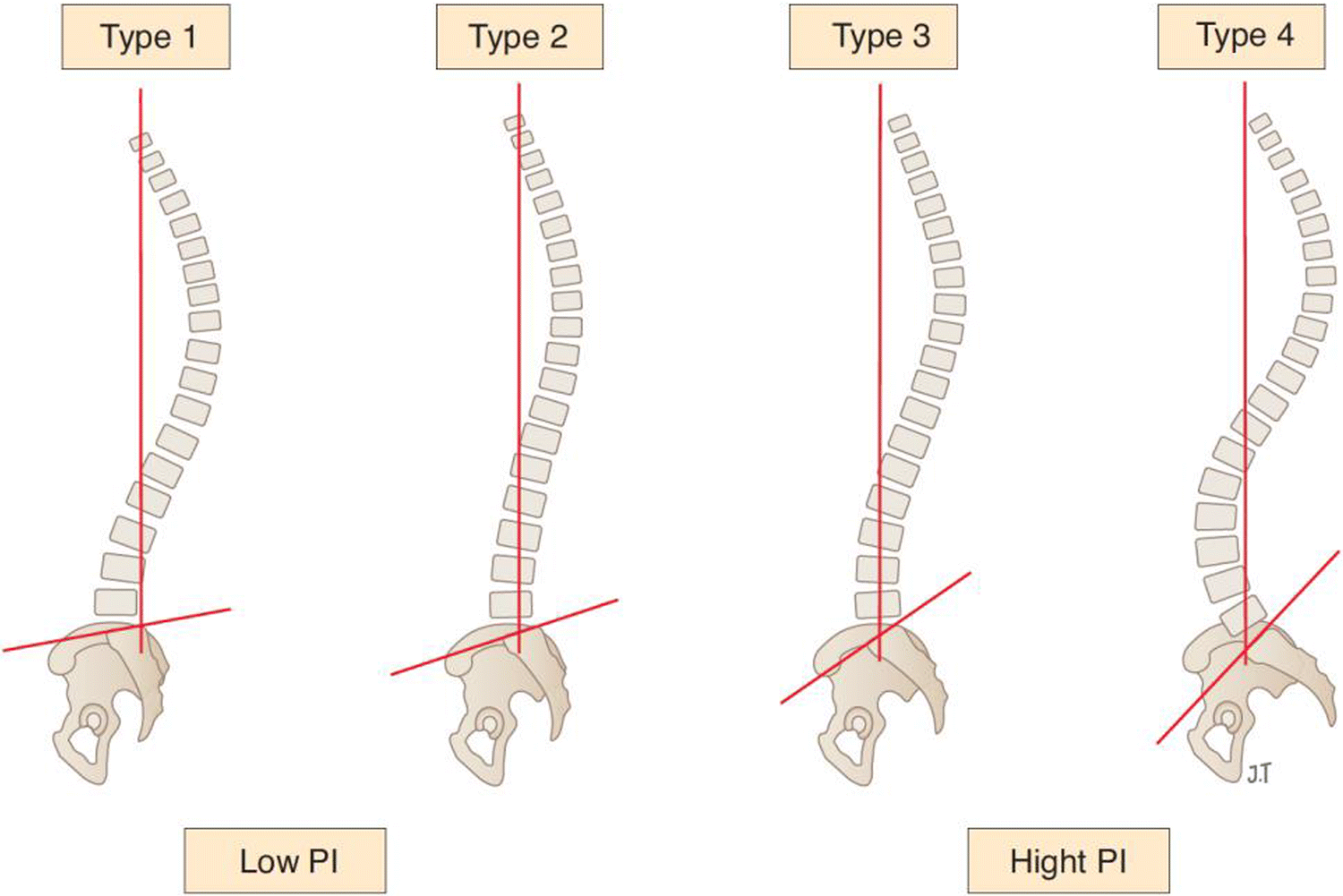
Types 1 and 2 are characterized by a small sacral slope (less than 35°):
Type 3 corresponds to an average sacral slope (between 35° and 45°) with a lordotic apex at L4. The lordosis is almost equally distributed over the two arches. This is the most balanced type.
Type 4 corresponds to a steep sacral slope (greater than 45°) with a lordotic apex at the anterior–inferior corner of L3. The global lordosis angle (LL) is larger and includes more vertebrae than the other types. The thoracic kyphosis is shorter.
Normative values in the asymptomatic population are very important to know to have a better analysis of the pathological situations.
Barrey et al. [20] were the first to grouped 154 asymptomatic volunteers, described pelvic and spinal parameters as a function of pelvic incidence. This study stratified the study subjects into 6 groups according to their pelvic incidence angle. However, the extreme groups did not have a sufficient number of persons to detect a statistically significant difference. The work of Le Huec and Hasegawa reinforces Barrey’s study with subgroups of sufficient size [9].
From these two studies, we can conclude that overall, for pelvic incidences below the average value (50°), lordosis angle tends to increase, while the incidence decreases, whereas when pelvic incidence is around 50°, the lordosis tends to equal the incidence angle value (LL = PI)), and when the incidence is over 65°, the lordosis tends to be less than the PI. Thus, the formula often used PI = LL + 9° is only valid for small incidence angles, which leads to numerous estimation errors when the pelvic incidence is greater than 50° [19]. This could be one of the reasons of overcorrection of lordosis when performing posterior substraction osteotomy in patients with high incidence angle.
The spine balance is a dynamic phenomenon, and therefore, it is important to analyse parameter variations due to ageing process and changes during daily activities.
Physiological spinal ageing begins with the degenerative loss of disc height and thus leads to loss of lumbar lordosis, which disrupts pelvic balance. Battié showed that 74% of disc degeneration is due to genetic factors [21]. With advancing age, the lumbar spine undergoes a number of modifications. These are then associated with disc mechanical incompetence (loss of elasticity, hypermobility, etc.), hypertrophy of the articular facets, bone remodelling and atrophy of the extensor muscles. These changes lead to a lumbar hypolordosis or kyphosis which may be the cause of an anterior sagittal imbalance [20, 21].
The modification of lumbar lordosis is directly related to degenerative phenomena. On the other hand, the modification of the other spino-pelvic parameters is linked to compensatory mechanisms which aim to maintain the upright position with minimal muscular effort so as to keep a horizontal gaze and the head over the pelvis.
Recently, Amabile [22] have showed that the OD-HA angle (odontoid hip axis angle), which characterizes the overall spinal balance, remains constant whatever the age and despite variations of lordosis (which decreases with loss of disc height) and the presence of compensation mechanisms.The four spino-pelvic types described by Roussouly have also different biomechanical characteristics and, as such, do not all show the same degenerative patterns (Fig. 8). Barrey et al. [20] showed that they represent different predisposing morphotypes:
The study of the changes in the spine during ageing makes it possible to show compensation mechanisms at three levels: spinal, pelvic and lower limbs. Understanding these different data allows for better planning of the surgical management of the patients. It involves the creation of an image of the entire spine and the measurement of the spino-pelvic parameters to determine, by integrating all these parameters, the extent of the correction to be performed during surgery. Taking these parameters into account also enables us to understand the complications involved in this type of surgery: transitional syndromes or junctional syndromes. It is also possible to integrate these parameters into the study of gait, an area still under investigation.
To adapt to the variations in the shape of the spine, several compensation mechanisms are implemented at the segmental, regional and global levels (Fig. 9) [23]. These mechanisms are not all implemented at the same time but are associated with different extents.
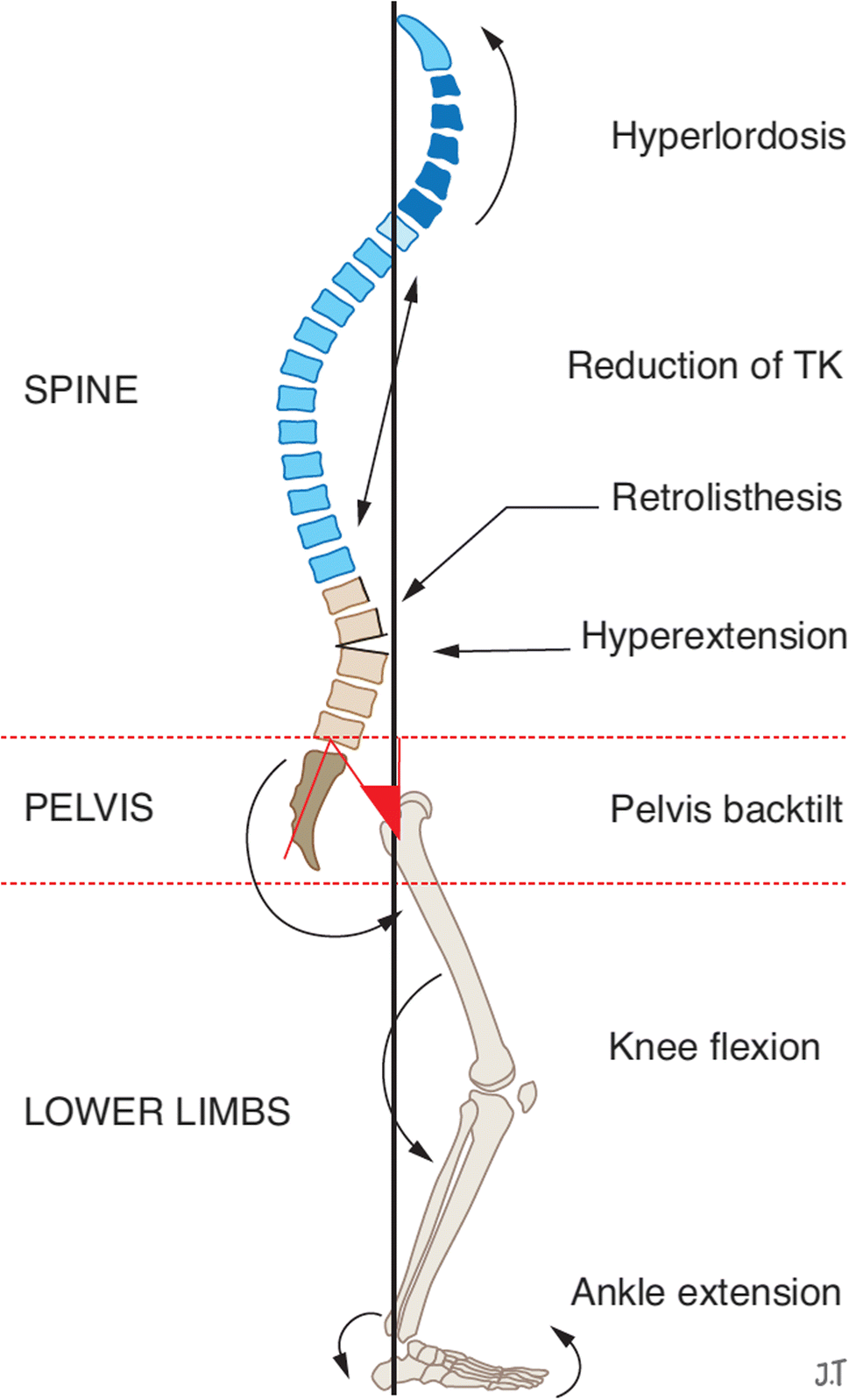
The basic concept of spinal compensation is the extension of the adjacent spinal segments in order to avoid the anterior translation of the gravity line due to progressive disc degeneration and loss of disc height. This, however, causes adverse effects.
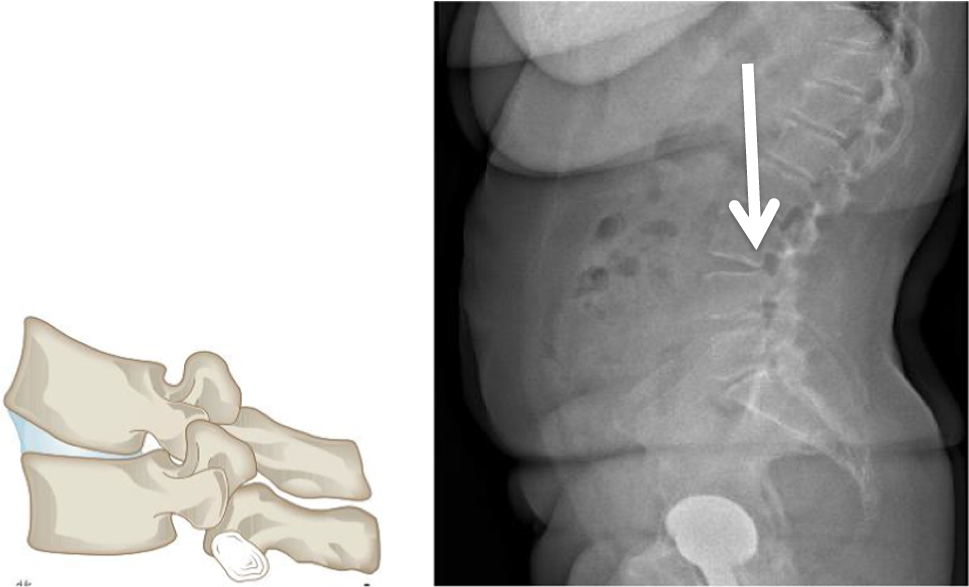
There is frequently hyperextension of adjacent segments at the lumbar level: This hyperextension can be mono- or multi-segmental and is defined by a single segmental lordosis above 15°. This mechanism causes an increase in posterior stresses and results in retrolisthesis, facet hypertrophy and excessive pressure on the spinous processes (Baastrup syndrome). This also can reduce the diameter of the intervertebral foramen and central canal. An indicator worth noting is the “leaning back sign” described by Faundez et al. [24] and characterized by a hyperextended disc with anterolisthesis at the same level: The upper vertebra is slipped forward and leaning in hyperextension on the vertebra below (Fig. 10).
The sole mechanism at the level of the pelvic is retroversion. It corresponds to a posterior rotation of the pelvis around the femoral heads, translated in an increase in pelvic tilt and a decrease in sacral slope. Pelvic retroversion translates into extension of the hip joints. Several studies have shown that chronic low back pain patients have a retroverted pelvis [15]. The higher the value of the pelvic incidence, the greater the retroversion can be. This is caused by contraction of the extensor muscles of the hips (gluteal muscles) [25, 26]. The range of hip extension between the natural upright position (normal population) and that of maximum extension (pelvic retroversion) can be considered as the “extension reserve” A well-functioning spine requires this hip extension, allowing it to assist in the compensation of sagittal imbalance [27, 28]. Hovorka has proposed methods of radiographic measurement of this hip extension reserve [27]. Lazennec also proposed a measurement using the EOS imaging system [28]. The hip extension reserve is included in the pelvic retroversion capacity. This represents only few degrees, but those are important to know as this possibility is missing in case of hip arthrosis leading sometimes to limited retroversion in case of hip flexum [27].
Another regional compensation mechanism is knee flexion, which usually happens after maximal pelvic retroversion has been reached.
The decrease in thoracic kyphosis usually observed in younger subjects because it results from the contraction of erector muscles, which are still strong and efficient.
Cervical hyperlordosis also results from the contraction of erectors muscles in the cervical spine and can eventually produce facet joint hyperpressure, arthritis with foraminal or central stenosis (myelopathy). The forehead posture is an important compensatory positioning of the cervical spine allowing to keep the cervical foramen size open and allowing to keep the gaze horizontal by limiting cervical lordosis using the O-C2 hyperlordosis as a compensation (Figure 5 b). E Ferrero [29] showed also that the cranial sagittal vertical axis (Cr SVA) is a better radiographic measure to predict clinical outcomes in adult spinal deformity surgery than the C7 SVA.
Knee flexion and ankle stretching also help in shifting the line of gravity backwards. Knee flexion has been shown to be correlated with loss of lumbar lordosis [22]. Considering the feet as the base of support, one compensatory mechanism to keep the head and the gravity line in good position is the concept of pelvis translation as shown by Ferrero [29].All these mechanisms combine in different ways depending on the person. This compensation is of limited efficiency, especially in elderly persons, who have a weakened musculature and often arthritic joints (Fig. 11). To integrate all those compensatory mechanisms in a new balance concept to complete the Dubousset’s conus of economy, we proposed to use the new 3 conus concepts in order to split the analysis at each level and have a better analysis of the global balance. The lower conus includes the lower limb and the femoral head. The median conus includes the pelvis and the thoraco-lumbar spine up to T1, and the upper conus includes the cervical spine and the head. Each conus can adapt its compensatory mechanisms but always in a way to keep the head over the 2 feet base of support [30] (Fig. 11 bis).
How do we integrate these data before treating those patients or during surgical planning before spinal surgery? The goal is to move in two steps:
Several indicators have therefore been defined so as to evaluate the overall spinal balance. All this can be evaluated only by obtaining full spine radiographs on large cassettes or with the EOS low-dose imaging system (EOS imaging, Paris, France) [12].
Radiography of the entire spine is mandatory. The analysis of sagittal balance requires radiographic anteroposterior and lateral views of the entire spine in standing and relaxed positions, from C2 to the femoral heads. The position must also be standardized: hands resting on collarbones [31]. These radiographs can be made on large cassettes or with the EOS imaging system. The EOS imaging system enables us to produce images of the entire spine while considerably reducing the radiation dose (8–10 times less than standard radiology) and much faster than with traditional imaging systems [32]. The image capture is very fast, allowing also the 3D modelling. This system avoids the phenomena of vertical distortion found in large cassette imaging.
Overall assessment of balance can be performed using different parameters:
This is the lowered vertical line of C7. Ideally it must pass through the sacral endplate, but even if this is the case, it does not imply that the spino-pelvic parameters are adequate: The spine can be in (compensated) balance, but spino-pelvic parameters can be inadequate (not aligned).
The sagittal vertical axis [15, 33] (Fig. 13): Jackson also described the sagittal vertical axis or SVA which corresponds to the horizontal distance between the C7 plumb line and the posterior–superior S1 corner.

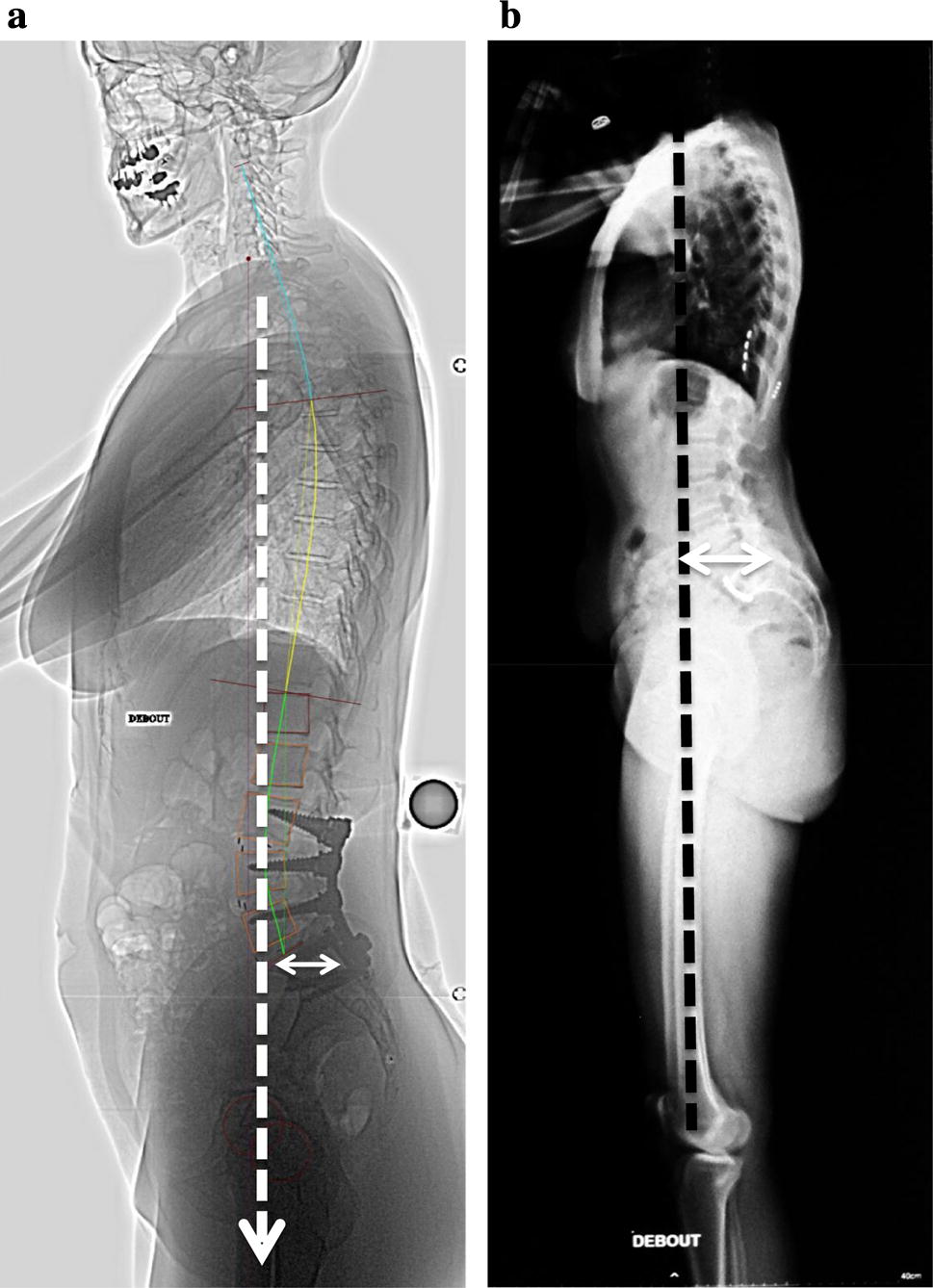
The SVA is correlated with quality-of-life parameters [34]. The normal SVA should be less than 5 cm, but this parameter is age-dependent [35]. However, in our opinion, it does not take into account the value of pelvic incidence, which induces considerable interpretation bias, particularly in high pelvic incidences. (The pelvis has a larger anteroposterior diameter in high pelvic incidence.) On the other hand, the average values are not very selective and only the subgroup stratification allows for an appropriate analysis of the balance. This parameter should be used only to compare the balance situation of a patient over time or before and after surgical treatment. It cannot be used to compare the results of a series of patients because their pelvic incidence angles are not the same, due to anatomical differences as explained above [20] (Fig. 14a, b)
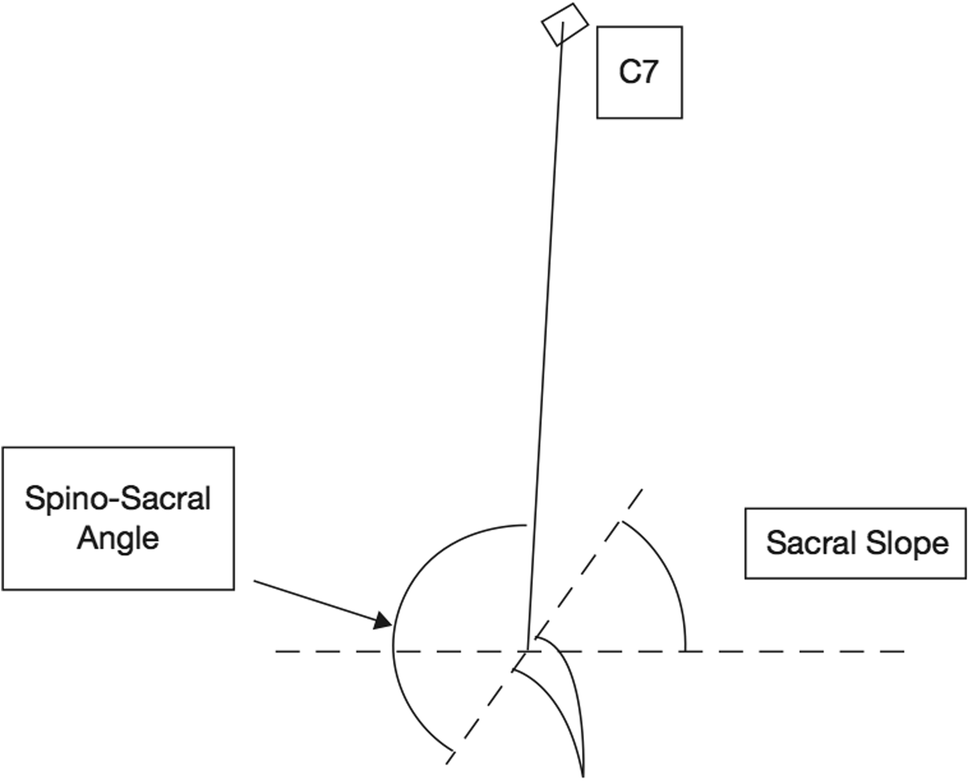
The SVA corresponds to a measurement of distance, so it requires calibrated images as opposed to indicators that use angles.Spino-sacral angle or SSA [20] (Fig. 15) is defined by the angle connecting the centre of the C7 vertebra to the centre of the S1 endplate and the line parallel to the superior S1 endplate. Its normal value is 135° ± 8°. This is an intrinsic parameter of balance [36]. It is a parameter of overall balance because it integrates the C7 position with a pelvic parameter: the sacral slope. It does not integrate the cervical spine and head.
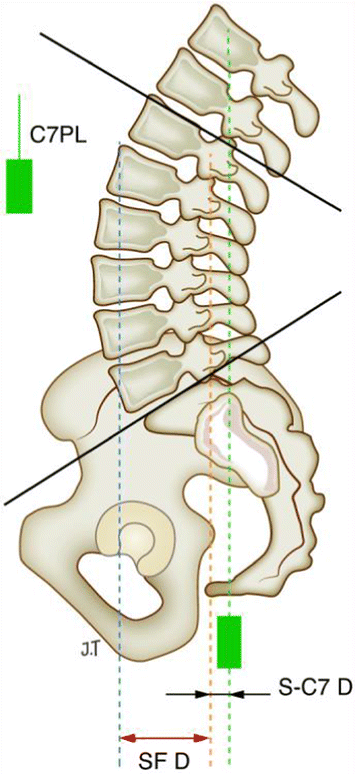
The purpose of the C7/SFD ratio (Barrey index) is to replace a distance parameter like the SVA by a ratio applicable to all radiographs and also take into account the position of the femoral head and therefore some of the thickness of the pelvis, which varies according to the angle of pelvic incidence [23].This ratio is equal to 0 when the C7 plumb line is projected exactly at the posterosuperior corner of the sacrum, and is equal to 1 when it is projected on the bi-coxo-femoral axis. It is greater than 1 when the C7 plumb line projects in front of the femoral heads and negative when the latter projects behind the sacrum (normal value is − 0.9 ± 1). It does not integrate the cervical spine and head (Fig. 16).
This corresponds to the angle between a line connecting the centre of T1 to the centre of the femoral heads and the line to the centre of the S1 endplate. It has been correlated with pelvic tilt and SVA, but does not account for pelvic incidence value. The TPA target value is < 14°
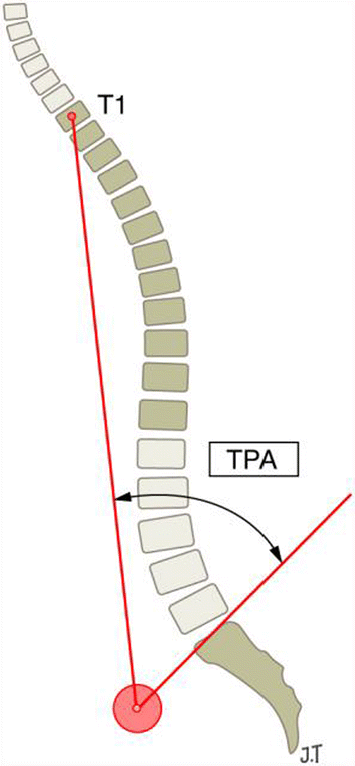
This is an angle somewhat similar to the SSA for thoracic–lumbar–pelvic analysis. It does not integrate the cervical spine and head.
Global tilt angle (GT) [38] described to analyse the balance takes also C7 as a landmark. It does not integrate the cervical spine and head. This angle is more interesting in sitting position.
This index estimates the extent of corrections to be performed on patients with spinal imbalance. The FBI technique is based on the overall analysis of sagittal balance including the lower limb position.
It is based on three parameters:
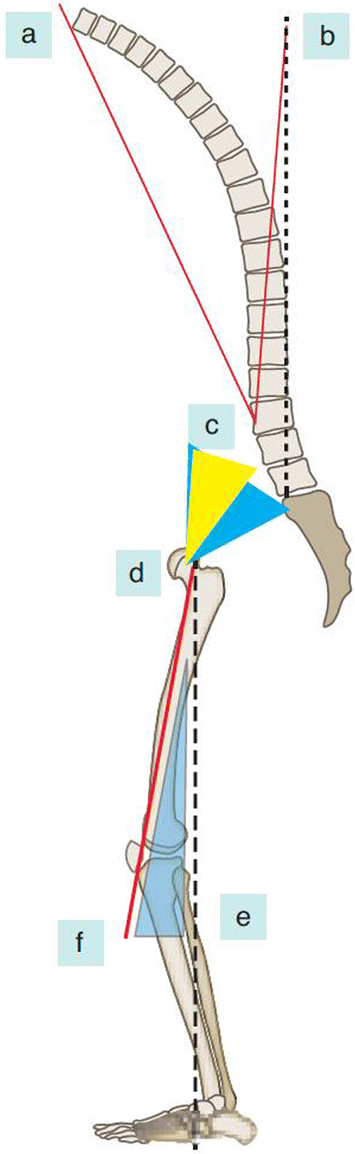
The FBI is calculated as follows: The first angle corresponds to the C7TA determined by: the centre of the inferior C7 endplate (a) which is transposed horizontally on the “ideal” C7 vertical projection (b) which is on the axis of the posterosuperior S1 corner and the apex of the angle is L4 vertebra. In the normal population, the apex of the lumbar lordosis is located mostly around L4. These three points (centre of C7, “ideal” C7 and L4) form a triangle whose apex is the L4 vertebra.
The sum of these three measurements gives the value of sagittal angle correction required to restore a balance adapted to the patient. However, this technique can also be used to analyse the overall balance. Its average value in asymptomatic people is less than 5° [39] and could be negative. It does not integrate the cervical spine and head.The OD-HA (odontoid hip axis) [40] (Fig. 19a, b): This is the angle between the vertical and the highest point of the odontoid process (dens) connecting to the centre of the acetabulum (bi-coxo-femoral axis). This angle was studied in an asymptomatic patients subgroup (SD: 1,6°). It hardly varies and is a good way to study the overall sagittal balance. It integrates the cervical spine and head and stays constant even in elderly if they are asymptomatic.
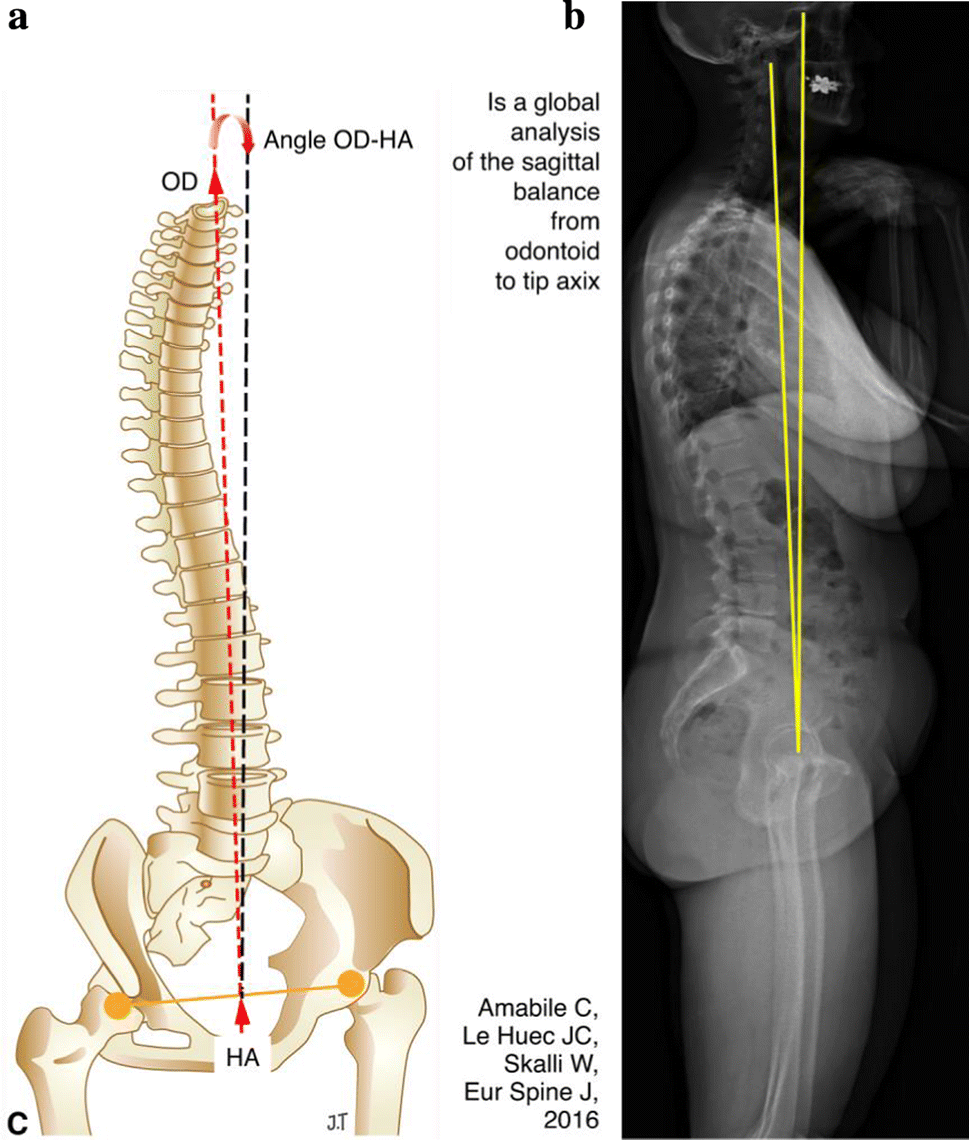
This angle takes into account the position of the cervical spine, the thoraco-lumbar spine and pelvis, and may benefit an overall analysis and assessment of the risk of proximal junctional kyphosis (PJK) after an extended thoraco-lumbar fusion. In fact, if OD-HA is positive (>+ 2°), above the normal value (+ 2° to − 5°), it means that the patient is out of balance, and there is an increase in the lever arm on the upper instrumented vertebra (UIV), as shown in the study by Faundez et al. [13].
Preoperative planning is today mandatory before any kind of spine fusion to avoid overstress on adjacent levels as proposed by Berjano [41]
The junctional syndrome or proximal junctional kyphosis (PJK) is defined historically by a 10° increase in proximal junctional kyphosis compared to the preoperative radiograph [42]. This is measured between the inferior endplate of the first instrumented vertebra and the superior endplate of the second vertebra above it. This is the major complication in deformity correction surgery. Proximal junctional kyphosis often occurs early (within 3 months), in postoperative patients. There are risk factors which the surgeon can modify during surgery:
Several studies have shown the increase in mobility in the segment adjacent to the arthrodesis, which could explain its degeneration [47]. It is crucial to integrate the cervical spine and the head when analysing the PJK or PJF risk. The recently published CIA [13] (cervical inclination angle) (Fig. 5a) could provide a good help to predict the risk of junctional breakdown if its value is maintained around 85° for the first thoracic vertebrae in long construct up to T3 or T4.
Junctional breakdowns leading to PJK and subsequently to PJF are always worsened by a too important lever arm at the superior part of the body, located above the last instrumented vertebra. Therefore, it is mandatory to be able to evaluate this lever arm preoperatively by pre-op planning as proposed recently by Faundez [13] using software allowing to simulate the post-op correction and simultaneously with a second software to evaluate the lever arm and constraint applied at the upper instrumented vertebra (UIV). This way the construct can be longer or shorter according to the correction need and respecting the biomechanics to avoid excessive load at the UIV. This new way of thinking must be combined with preoperative control of spine correction during the surgery to be sure that the pre-op planning is fully respected during the operative procedure.
It is also important to study the overall sagittal balance during gait in pathologic conditions. Indeed, a balanced but compensated spine, on static radiographs, can become unbalanced when set in motion. Recently, Y Shiba has performed a three-dimensional gait analysis in patients with degenerative lumbar kyphoscoliosis [48]. He demonstrated that the loss of overall sagittal alignment was underestimated on static radiographs. Indeed, the anterior imbalance occurs, or increases, as soon as a step is made and progresses along that step (Fig. 20).

This is explained by the compensation phenomena incurring in an anterior imbalance. In fact, one of the first compensatory phenomena occurs at the level of the pelvis when the extensor hip muscles, which take part in pelvic retroversion, are activated. During gait, the hip extensor muscles does alternatively contract and no longer contributes to a static pelvic retroversion. This results in pelvic anteversion. The anterior imbalance is then no longer compensated and increases from the onset of the gait. The tendency to lean forward during gait is accentuated when the posterior spinal muscles have atrophied and no longer allow the trunk to be held vertically, a common condition in patients with degenerative kyphoscoliosis.
Lee, in his study of “flat” degenerative spines, separated two groups of patients according to their pelvic tilt, during gait [49]. The first group of patients maintained pelvic retroversion during gait, while the second group could not. These findings indicated that patients who could maintain pelvic retroversion during gait (approximately 80%) would be improved by surgical correction, unlike those who displayed dynamic pelvic anteversion.
Bae has recently proposed to make radiographs of the entire spine after a 10-min walk, so as to detect a major anterior imbalance that can or cannot be compensated on static radiographs [50].
These different concepts of sagittal balance allow for the analysis of the clinical condition of a patient. There are 3 types of profiles:
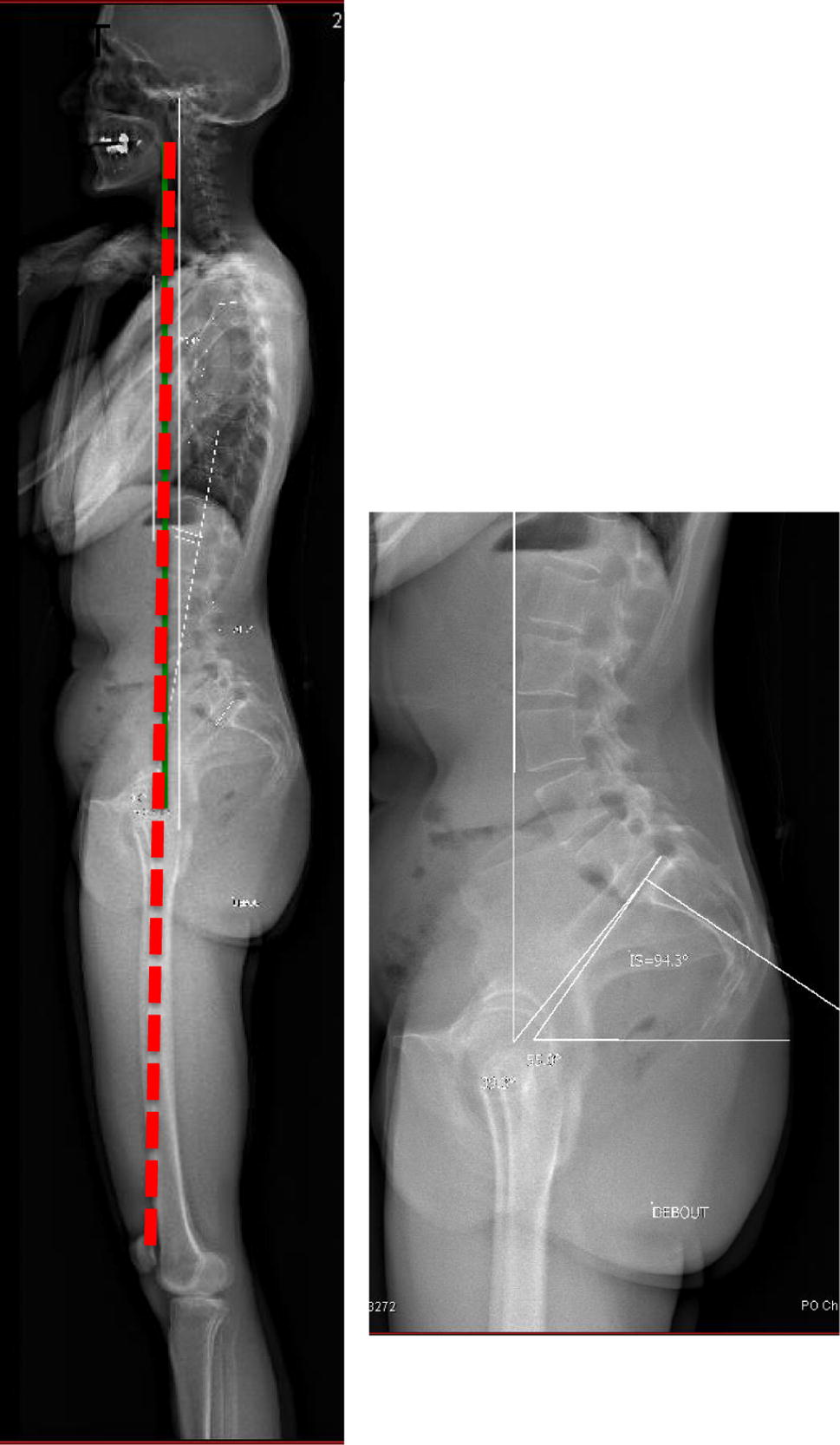
This analysis suggests a therapeutic strategy. In practice, it is important to know how to treat the pathology by adapting a strategy to each individual patient: taking into account certain general problems (cardiac, pulmonary, diabetic, obesity) and the patient’s ability to compensate. By allowing for a compensated balance, a simpler surgery is recommended, rather than major surgery with a high risk of complications [51]. Understanding sagittal balance provides the most appropriate choice [52]. Sagittal balance is a dynamic phenomenon, and it is better to have a good sagittal balance (even compensated) than a good sagittal alignment with a long fusion and no ability to compensate [39, 53]. This is the reason why we came to the conclusion that the recent papers providing rules to tolerate increased pelvic tilt and SVA in elderly is probably not appropriate. The only good way to prepare a spinal fusion surgery is to make a plan and simulate what will happen after a short or long fusion. Knowing all the parameters presented above and understanding the compensatory mechanisms that will allow for a good global balance, we suggest that using the OD-HA angle would be the best way to predict the risk of failure or junctional breakdown. The muscle function can be approximately evaluated on dynamic flexion/extension X-rays, in standing position and gait analysis after 10-min walking.Two examples of sagittal balance analysis (Figs. 21 and 22) show how to analyse the balance before any surgical treatment.
Sagittal balance of the spine is a vast subject which must be apprehended with the patient standing at rest in a standardized position, but also during walk, from which we can detect very harmful stresses on the osteoligamentous structures. The fundamental principles have been analysed on static standing radiographs, but in the future the study of gait will add fundamental information. Analysis of spino-pelvic parameters helps to guide the surgical strategy in spinal surgery. It is very useful in preoperative planning, but allows us also to understand what went biomechanically wrong after a surgery.
The global analysis including the cervical spine and head is nowadays mandatory. Sagittal balance must be carefully considered before any surgery, limited or not, and especially at the lumbar level and, above all, if the L4-L5-S1 levels (which represent 66% of the lordosis) are included in the fusion.
The authors declare that they have no conflict of interest.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
586_2019_6083_MOESM1_ESM.pptx (2.6 mb)Supplementary material 1 (PPTX 2662 kb)
© The Author(s) 2019
Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.