Due to a high prevalence of low back pain (LBP) among children and adolescents, it is significant to seek effective prevention and therapeutic procedures. One idea for the programmes is a potential relation between the occurrence of LBP and the level of physical activity. The aim of this review was to analyse the current knowledge regarding the association between physical activity and LBP among children and adolescents.
Publications were retrieved by searching the following databases: PubMed, The Cochrane library, Web of Science, Medline and SportDiscus with Full Text (EBSCO). The search strategy included keywords related to physical activity and LBP. The studies included were assessed for methodological quality. PRISMA guidelines were followed for the systematic review.
The total sample size of the nine included studies consisted of 75,233 subjects, with an age range of 9–19 years. All the studies were assessed to be of high quality. One cohort study and five cross-sectional studies found the association between physical activity and LBP in children and adolescents. The remaining studies found no relationship between physical activity and LBP. These findings showed that both extremes of activity levels (i.e. being very low and very high physically active) are associated with LBP.
There is moderate evidence for the association between physical activity and LBP in children and adolescents. The results highlight the need for continued research. It seems that for clear evaluation of the analysed association the prospective cohort studies should be conducted.
Epidemiological data have shown that low back pain (LBP) is not only a health problem for adults but is also frequently reported by schoolchildren [1,2,3,4,5,6,7,8,9,10,11,12]. The prevalence of LBP in children and adolescents increases with subjects’ age [13,14,15], and females demonstrate its higher occurrence [2, 7, 16, 17]. A recent study found that the self-reported prevalence of LBP was 31%, 51.9% and 71.2% among children aged 10–13, 14–16 and 17–19 years, respectively [11]. Back pain during this period of life may have health implications in adulthood [18, 19]. The high prevalence and care seeking translate into a substantial financial burden for society. In the USA, the annual cost of chronic pain in adolescents aged 10–17 years, of which musculoskeletal pain comprised the largest proportion, was $19.5 billion [20]. In Germany, a minimum figure for direct costs for the treatment of people under the age of 25 years with back disorders is €100 million per year [21]. Given this, understanding the relation between main factors associated with LBP and prevalence of LBP is crucial.
The aetiology of back pain in children and adolescents is unknown. And furthermore, studies investigating risk factors for LBP report mostly unclear associations [22]. Studies revealed that physical activity is one of the important factors related to the risk of back pain in children and adolescents, and being physically active may be important in the prevention and management of LBP [23, 24]. On the other hand, there is evidence that heavy physical activity is hazardous on the back [25, 26].
The last systematic review based on the analysis of the relation between physical activity and LBP in schoolchildren was published in 2011 [27]. This review showed conflicting evidence for the association between physical activity and LBP occurrence in schoolchildren. Therefore, the analysis of the current research seems to be important to improve understanding of physical activity-related risk factors for LBP and may be important in the prevention and management of LBP in children and adolescents.
The aim of this review was to analyse the current knowledge regarding the association between physical activity and LBP among children and adolescents.
Publications were retrieved by searching the following databases: PubMed, The Cochrane Library, Web of Science, Medline and SportDiscus with Full Text (EBSCO). The search strategy included keywords related to physical activity and LBP. An example of the search strategy for the PubMed database is provided in Table 1. All articles published between 2011 and December 2019 were eligible for inclusion in the review.Table 1 Search strategy (PubMed)Full size table
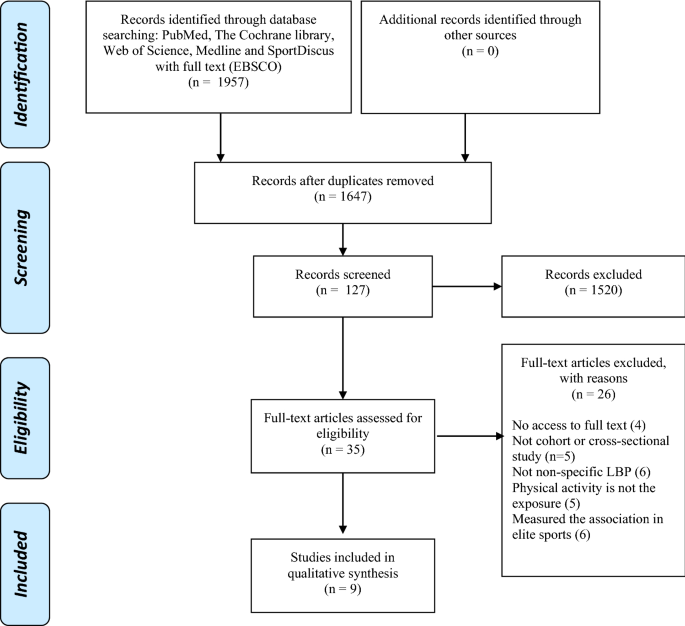
The information sources were searched independently by two reviewers (AK and MP). The reviewers screened the identified papers and made decisions about inclusion according to the eligibility criteria. Disagreements were resolved by consensus or a third reviewer (DC). All citations were screened to identify relevant studies, firstly by title, secondly by abstract and thirdly by full-text screening. A paper was considered potentially relevant and the full text reviewed if, following discussion between the two independent reviewers, it could not be unequivocally excluded on the basis of its title and abstract [28]. The number of articles included and excluded at different phases was presented in a PRISMA flowchart (Fig. 1). PRISMA guidelines were followed for this systematic review [29].
The studies were included if they met the following criteria:
Studies were excluded if they:
Data were extracted independently by two reviewers (AK and MP). Disagreements were resolved through discussion between the reviewers. The extracted data included first author, year of publication, study design, study population, participant characteristics, sample size, LBP measurement tool and prevalence of LBP, physical activity type, physical activity measurement tool and main findings. The corresponding authors of eligible studies were contacted if potentially relevant data were missing.
The studies were assessed for methodological quality using modified checklist for quality appraisal from the previous systematic review [24]. The assessment was carried out by two reviewers (AK and MP) independently. Preceding the final screening, reviewers pilot tested the methodological quality assessment of two similar articles that were not included in this review. Disagreements were resolved by discussion or consultation with the third reviewer.
Different checklists were used for the quality assessment of different study designs (Table 2). Sixteen criteria were used to assess the methodological quality of cohort studies, and 14 criteria were applied for cross-sectional studies. Each item was rated as positive or negative (potential bias) or unclear (if description was unclear). Each study was assigned a total score, which was the sum of all positive ratings according to the methodological criteria. The reviewers considered studies to be of high quality if the methodological quality score was more than 50% of the maximum score [30]. Therefore, cohort studies scoring more than 8 and cross-sectional studies scoring more than 7 were identified as high-quality studies. Only high-quality studies were included in the review.Table 2 Methodological quality assessment of the nine studiesFull size table
The strength of evidence was divided into five levels based on the study design, the number of studies and the quality score of studies [30]:
Cohort studies and cross-sectional studies were assessed separately. To analyse association between LBP and physical activity, the relationship between these factors was explored and pooled if methodological homogeneity in the studies was identified. This involved making a subjective decision based on consensus between the authors. Key factors in this decision included study population, type of exposures and outcomes measured, methods of exposure assessment and data presentation. The analysis of the results was limited to qualitative summary.
The searches retrieved 1957 studies. After removing duplicates, 1647 studies remained. Based on the analysis of the titles and abstracts, 35 studies were eligible for assessment by full paper. Of these, nine studies [31,32,33,34,35,36,37,38,39] fulfilled the inclusion criteria for further analysis.
The included studies comprise two cohort studies [31, 35] and seven cross-sectional studies [33, 34, 36,37,38,39]. For cohort studies, the shortest follow-up period was 2 years [31] and the longest 6 years [35]. The flow of studies through the review is depicted in Fig. 1.
The total sample size of the nine included studies consisted of 75,233 subjects (ranging from 144 to 31,429 participants), with the age range of 9–19 years. All studies recruited both females and males. The characteristics of the included studies are described in Table 3. It was not possible to pool data due to heterogeneity regarding exposure (physical activity) and outcome (low back pain) measures.Table 3 Characteristics of the included studiesFull size table
The majority of the included studies (n = 8) used questionnaires to measure physical activity level, and only one study used objective measurements of physical activity (GT3X triaxial accelerometer) [31]. Six studies examined leisure-time physical activity [33,34,35,36,37, 39]. Three studies assessed daily physical activity [31, 32, 38]. All of the included studies adopted different classifications of physical activity levels taking into account the intensity of physical activity, the frequency of physical activity each week and the average time of each physical activity.
The prevalence of LBP episodes was measured by the use of a questionnaire [31,32,33,34,35,36,37,38,39], of which two studies used standardized Nordic questionnaire [32, 38]. In six of the studies, the authors gave information on the validation and/or reproducibility of the questionnaires [31,32,33,34, 38, 39].
Associations have been most widely expressed by odds ratios or relative risks.
The scoring of the two reviewers of the included studies had an agreement rate of 91% (29/32) for cohort studies and 89% (88/98) for cross-sectional studies. All disagreements were resolved during a consensus meeting. The results of the methodological quality appraisal are presented in Table 2. For the cohort studies, the mean score for methodological quality was 75%. The mean score for methodological quality of cross-sectional studies was 68% with a range of 57–79%. Two cohort studies were rated as high-quality studies. Seven cross-sectional studies were rated as high-quality studies. All the studies that were eligible to be included in the analysis were assessed to be of high quality.
One cohort study showed that objectively measured physical activity (using the accelerometer) in 11–13-year-old adolescents was generally not predictive of LBP prevalence [31]. Proportion of the day spent at different physical activity levels did not predict the incidence of spinal pain. Physical activity did not affect the risk of spinal pain, but the 10% most active adolescents were at increased risk of developing spinal pain. Thus, vigorous physical activity appears to be a risk factor for spinal pain in adolescents [31]. The other cohort study found an association between activity and LBP [35]. LBP was more prevalent in the extracurricular sports activities group than in the non-extracurricular sports activities group in almost every grade, regardless of gender [35]. The results from cohort studies are summarized in Tables 3 and 4.Table 4 Results from studies included in the reviewFull size table
Five studies found an association between physical activity and LBP in children and adolescents [34, 36,37,38,39]. Two studies [34, 38] reported that a low level of physical activity is a risk factor for LBP occurrence. Another study found that the group who engaged in physical activity 1–4 times weekly showed significantly less LBP than those who did so for longer or shorter periods [39]. And moreover, three studies [36, 37, 39] found that a high level of physical activity is associated with high prevalence of LBP. One study found that children who spent ≥ 4 h per week doing sport were more likely to have lifetime LBP [36]. Another study reported that the group that exercised for approximately longer that 2 h each day showed significantly more often prevalence LBP than those who did so for shorter periods [39]. The results from cross-sectional studies are summarized in Tables 3 and 4.
Of seven high-quality cross-sectional studies, two studies did not find an association between LBP and daily physical activity [32] or leisure-time physical activity [33, 37].
To sum up, there was moderate evidence for the association between physical activity and LBP.
In this review, we explored the most recent literature on the association between physical activity and LBP occurrence in schoolchildren. In the final analysis, we have included nine studies. Evidence from two cohort studies supported the findings from seven cross-sectional studies. This systematic review provides moderate evidence for the association between physical activity and LBP in children and adolescents. One cohort study [35] and five cross-sectional studies [34, 36,37,38,39] found an association between physical activity and LBP in children and adolescents. The remaining studies (n = 3) found no relationship between physical activity and LBP.
These findings showed that both extremes of activity levels (i.e. being very low and very high physically active) are associated with LBP. Our results correspond to the results in the study by Heneweer et al. [25]. They concluded that the correlation between back pain and physical activity may be U shaped. Both a sedentary lifestyle and high-intensity physical activity increased the risk of back pain. The authors concluded that it was the quality, not the quantity of physical activity that was significant [25]. It is possible that different dimensions of recreational and sport-related activities may have different relationship with LBP. It seems that some types of sports can be beneficial or harmful in developing or protecting against LBP in children and adolescents. Sports activities are characterized by a mixture of different back loading forces, so specific sport activities may be detrimental to the spine. The risk of LBP associated with intensive sports practice during childhood should be explored in future studies.
Based on the limited number of studies and their heterogeneity, the results indicated moderate but not strong evidence for the association between physical activity and LBP.
One of the possible explanations for inconsistent findings among studies may relate to heterogeneity in methods of exposure assessment among studies. Most of the included studies focused on physical activity only at leisure time, which may not reflect actual daily physical activity. Physical activity during PE should be assessed and included as part of daily physical activity. Only three studies [31, 32, 38] focused on the association between daily habitual physical activities and LBP. And furthermore, a variety of PA measures were used. Most of the studies under examination used questionnaires in measuring physical activity that may produce recall bias in the estimation. To assess the physical activity level in participants with musculoskeletal pain, an objective measure is a preferable measurement device to self-report measurement [40]. Only one out of nine included studies used objective instrument (accelerometer) to assess physical activity level [31]. One of the problems is that objective methods were found to report different results than those obtained from subjective methods. Measurements and classifications of physical activity in terms of frequency, intensity and duration differed across the studies, which may lead to the misclassification of physical activity levels. The intensity of the physical activities must be further clarified with future research.
Another issue is related to the definition of LBP and validity of the exposure measurement. Only two studies provided a definition of LBP [32, 36]. In 5 studies [31,32,33, 38, 39], a diagram showing the location of LBP was used, which, in the case of younger children, is indispensable for better understanding of the question and providing a proper answer. The studies qualified for the review dealt with a very broad period of the occurrence of LBP. The studies asked about the occurrence of LBP in the period of the last 7 days [38], in the last month [33], the last 3 months [34], the last 6 months [39] and the last year [32]. In three studies, the question regarded whole life span [36, 37] or a current state [35, 37]. One study did not include information in which period LBP occurrence was analysed [31]. Different definitions of LBP may also result in various estimates of prevalence. Moreover, a large proportion of studies did not provide variables characterizing LBP (e.g. gender, intensity, frequency), or the inclusion or exclusion criteria for a group with LBP and without LBP. Most studies in this review did not divulge whether participants with spinal diseases which may cause LBP were excluded from the study. We therefore suggest that future studies should specifically exclude these participants. Moreover, all the included studies used questionnaires in measuring the occurrence of LBP. In most studies, self-administered questionnaires were used. In two studies, information on symptoms was collected with the standardized Nordic questionnaire (or adaptation thereof) for the analysis of musculoskeletal symptoms and this questionnaire has been considered an international standard [41]. Seven studies used a validated questionnaire [31,32,33,34, 38, 39].
Our results correspond to the results in the review by Sitthipornvorakul et al. [27]. Previous review showed conflicting evidence for the association between physical activity and LBP [27]. There is still no strong evidence for association between physical activity and LBP in children and adolescents.
There are some limitations associated with this review. First, most included studies used self-administered questionnaires in measuring physical activity that likely produce recall bias in the estimation. Second, it is noteworthy that definitions of LBP varied widely. Moreover, we summarized the results from studies with substantial heterogeneity. We found heterogeneity among studies as to aspects such as study design, study population, type of exposures and outcomes measured, methods of exposure assessment and data presentation which may limit the final conclusions. Finally, the search strategy was limited only to fully reported publications in English.
This is the first review in focused not only to the heterogeneity regarding the measurement of physical activity which was highlighted in previous systematic reviews, but also to heterogeneity of the analysis of LBP prevalence. In this review, we focused on data from cohort studies that investigated physical activity characteristics and the risk of low back pain, yet also included cross-sectional studies to capture all possible relevant information on the topic. This systematic review is based on the sensitivity analysis of only very high-quality studies. The strength of evidence was divided into five levels.
Based on the evidence from two cohort studies and seven cross-sectional studies, there is moderate evidence for the association between physical activity and LBP in children and adolescents. The results highlight the need for continued research. It seems that for clear evaluation of the analysed association the prospective cohort studies should be conducted. The design of future studies may be improved by taking into account a number of methodological limitations that are present in the published review.
Not applicable.
The authors received no specific funding for this work.
AK, MP and PK designed the research; AK and MP performed the research; AK, MP and DC analysed the data; AK, MP and PK wrote the paper; DC supervised the paper; and all authors read and approved the final manuscript. The authors have read the PRISMA 2009 Checklist, and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
Correspondence to Magdalena Plandowska.
The authors declare that they have no conflict of interest.
Not applicable.
Not applicable.
Not applicable.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.