February 2019, Volume 28, Issue 2, pp 234–240| Cite as
Lagerstrand, K., Hebelka, H. & Brisby, H. Eur Spine J (2019) 28: 234. https://doi.org/10.1007/s00586-018-5824-5
The aim was to (1) verify our previous finding that endplates (EPs) display load-induced T2-changes, (2) investigate whether vertebrae display load-induced T2-changes and (3) investigate whether EPs and vertebrae in LBP patients and controls display T2-differences during conventional unloaded MRI and axial loaded MRI (alMRI).
Twenty-seven patients (mean 39 years) and 12 (mean 38 years) controls were examined with T2-mapping on a 1.5 T scanner during conventional unloaded MRI and subsequently during alMRI (Dynawell® loading device), separated by approximately 20 min. For determination of EP and vertebral T2-values, volumetric regions of interest were manually segmented. Each vertebra was then divided into half to obtain superior and inferior units. The presence of EP changes (visual inhomogeneity in the EP zone), Schmorl’s nodules and Modic changes were registered.
For conventional unloaded MRI, the T2-values in the superior and inferior vertebral units and the EPs were significantly higher in the patients compared with controls (p < 0.03, p < 0.006) even when adjusted for the presence of Modic changes, Schmorl’s nodules and EP signal changes. alMRI induced significant changes in the superior EPs of the patients (p < 0.001). Additionally, the T2-value differed significantly between the superior and inferior EP, as well as between the superior and inferior vertebra with higher values in the inferior units (p < 0.001).
This study demonstrated significantly higher EP and vertebral T2-values in LBP patients in comparison with controls. In addition, alMRI induced significant T2-changes in the superior EPs for patients but not for controls. Importantly, the T2-differences between the groups may indicate that EPs and vertebrae in LBP patients have altered biodynamical characteristics compared to controls and the higher T2-values measured in patients may represent early inflammation or impaired nutritional transport.
These slides can be retrieved from electronic supplementary material.
Endplate Vertebrae T2-mapping Low back pain MRI
The online version of this article ( https://doi.org/10.1007/s00586-018-5824-5) contains supplementary material, which is available to authorized users.
Low back pain (LBP) is an endemic disease that causes more global disability than any other condition and is a well-documented source of chronic disability for both genders in their working years [1]. Intervertebral disc (IVD) degeneration, which involves biochemical changes with loss of proteoglycan and water content, structural changes with annular tears and herniation, as well as metabolic changes with reduced matrix synthesis, is associated with LBP [2]. Endplate (EP) changes and the presence of Modic changes in the vertebra are also known to be part of the degenerative cascade and are both associated with LBP [3, 4]. However, their association with intervertebral disc (IVD) degeneration is not fully elucidated. Neither is their relation to compromised EP function. In order to deepen the understanding of the pathophysiology behind these conditions, non-invasive diagnostic tools with the ability to detect early biochemical changes in EPs and vertebrae are desirable.
With the implementation of new magnetic resonance imaging (MRI) methods for functional characterization, detection of early biochemical changes in the EPs and vertebrae may now be feasible. T2-mapping, which is sensitive for alterations in composition between macromolecules, collagen and water and has been shown to reflect changes in biochemical composition and structural integrity in degenerated IVDs [5], may have the feasibility to reveal also comprised EP and vertebral functionality and therefore deepen the understanding of the pathophysiology behind IVD degeneration and LBP. Some studies have investigated the functionality of the EPs with T2-mapping and showed subtle deterioration of biochemical EP composition [6, 7]. At present, however, no work has characterized the vertebral tissue with T2-mapping. In addition, no work has investigated the value of EP and vertebral T2-mapping for differentiation of LBP patients from controls.
Axial loading of the spine has been shown to affect the IVD, where differences in the MRI signal between unloaded and loaded spine have been shown to display dynamic functionality [8, 9, 10, 11, 12, 13]. Also, new functional properties of the EPs and vertebrae may be displayed when the spine is loaded during MRI (alMRI), compared to conventional MRI that is performed with the spine unloaded (uMRI). In a small cohort study, we have shown that alMRI affects EPs in patients differently than in controls [14]. At present, no work has previously studied the dynamic behaviour of Modic changes. In particular, Modic type I changes have been pointed out as a potential marker of LBP [15]. Modic type I changes indicates hyper-vascularized inflammation that are associated with oedema and, as such, may be affected by alMRI. Hence, Modic type I changes may have a dynamic behavior displayed by alMRI.
The aim of this work was (1) to verify that EPs display load-induced changes measured with T2-mapping, (2) to investigate whether vertebral tissue display load-induced changes measured with T2-mapping and (3) to investigate whether EPs and vertebrae in LBP patients and controls display functional differences measured with T2-mapping during uMRI as well as during alMRI.
The study comprised 27 patients with chronic LBP (12 males, mean 39 years, range 25–69 years) that were included consecutively among patients referred to the radiology department with non-specific LBP. LBP were ensured using the standardized tools VAS, ODI, SF36 and EQ 5D. However, these were not further analysed as part of the study. Inclusion criteria were LBP for more than 6 months, clinically severe enough to be considered for surgery and age between 20 and 70 years.
For comparison, 12 age-matched controls were included (7 males, mean 38 years, range 25–63 years). Inclusion criteria for the controls were: age between 20 and 70 years, total absence of any type of LBP during the past 6 months and lack of previous LBP with duration more than 1 week. None of the participants suffered from any known medical history of back pain or spine-related disease.
Exclusion criteria for both patients and controls were previous spine surgery and contraindications for MRI. In total, 282/119 (patients/controls) EPs, and corresponding vertebral units, were examined.
The study was conducted according to the Declaration of Helsinki. Ethical approval was given by the regional ethics review board, and oral and written informed consent was obtained from all participants.
All MRI examinations were performed at daytime, between 9:00 a.m. and 15 p.m. using a 1.5 T MRI scanner (Magnetom Aera, Siemens Erlangen, Germany) with both the posterior and anterior phased array coils applied for increased signal-to-noise ratio. Conventional spine imaging was performed using optimized standardized sagittal T1- and T2-weighted MRI in the sagittal view (Table 1). T2-weighted imaging was also performed in the axial view. Moreover, functional T2-mapping of the spine covering L1–S1 was performed in the sagittal view.Table 1
MRI protocol, including T1- and T2-weighted MRI in sagittal view, T2-weighted MRI in axial view and T2-mapping in sagittal view
| Orientation | Field of view (mm) | Scan matrix | Slice thickness (mm) | NEX | |
|---|---|---|---|---|---|
| T1W MRI | SAG | 300 × 300 | 320 × 320 | 3.5 | 2 |
| T2W MRI | SAG | 300 × 300 | 384 × 384 | 3.5 | 1 |
| T2W MRI | AX | 220 × 220 | 256 × 256 | 3.5 | 1 |
| T2-mapping | SAG | 220 × 220 | 256 × 256 | 3.5 | 1 |
All participants were examined twice with the present MRI protocol, initially with uMRI and subsequently with alMRI. T2-mapping was performed at the end of the protocol, approximately 20 min after the first measurement. Hence, the spine had been unloaded/loaded for 20 min before T2-mapping was performed.
The alMRI measurements were performed with a Dynawell compression device (Dynawell diagnostics AB, Las Vegas, NV, USA) with load, corresponding to 50% of the body weight [8].
All post-processing of the images was performed with the dedicated analysis tool of the MRI scanner (Syngio Via, Siemens Erlangen, Germany). For reconstruction of T2-maps, optimized fitting of the raw data was performed to calculate the T2-value on a pixel-by-pixel basis. The images were then reformatted into 10 mm non-overlapping slices, where the three central slices were used in the analysis, thus covering 30 mm of the EP and vertebral width.
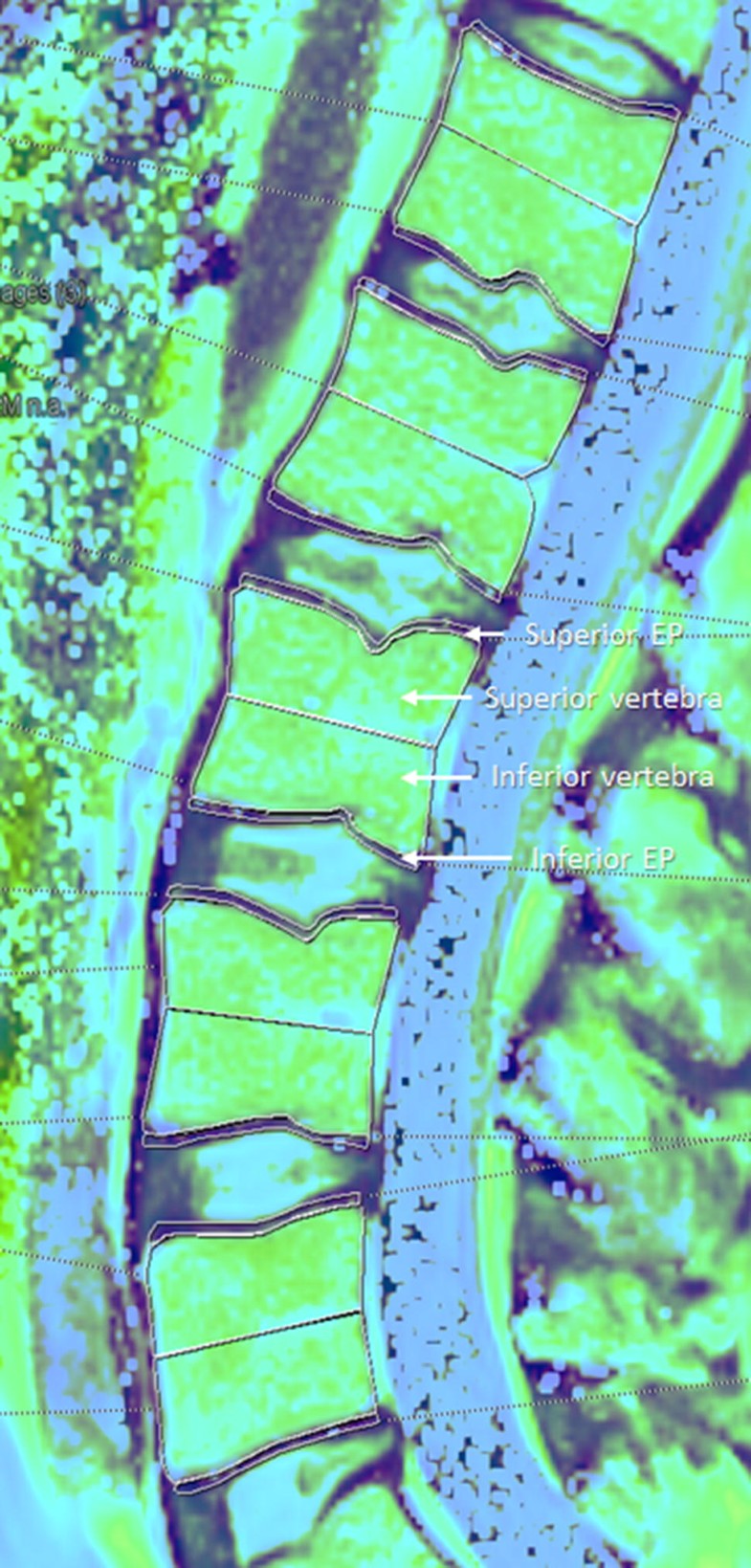
Disc degeneration was graded by an experienced radiologist, according to the Pfirrmann classification. The grading was based on the uMRI scans using all images in the image stack. Also, the presence of EP changes (apparent visual inhomogeneity, discontinuity in signal in the EP zone), Schmorl’s nodules and Modic changes were registered in the conventional uMRI images by the radiologist.For determination of mean EP and vertebral T2-value, the T2-maps were manually segmented into regions of interest (ROI) covering the EP zone and the vertebral body (Fig. 1). The EP ROI was positioned approximately one pixel away from the visible edge of the IVD and vertebral body, where the EP zone was assumed to include both bony and cartilage EP. The vertebral ROIs were subdivided into two parts to determine superior and inferior T2-values. Comparisons in T2-values between patients and controls for uMRI, alMRI and alMRI-uMRI were then performed.
All segmentations were performed by an experienced observer. Interobserver analysis was performed by repeating a subsample of the T2-measurements (all EPs and vertebrae in three different subjects). For intraobserver analysis, the same subsample was repeated by a second observer after extensive training.
All statistical analyses were performed using SAS Software version 9.4 (SAS Institute Inc., Cary, NC, USA). Categorical variables were expressed by number and percentage and continuous variables by median and standard deviation (SD). For comparison of T2-values between groups and difference between uMRI, alMRI and alMRI-uMRI within each group, a mixed linear model was used that adjusted for multiple observations within subjects. Comparisons between EP and vertebral T2-values were performed with correction for Schmorl’s nodules, EP changes, Modic changes and Pfirrmann grade. Results from models are presented as adjusted means (with 95% CI) and p value. Reliability of quantitative measurements for inter-rater agreement was performed using intraclass correlation coefficients (ICC) with 95% confidence intervals. The ICC model 2 was used with single measurements to determine consistency in agreement. The coefficients were interpreted according to Landis and Koch. All tests were two-tailed and conducted at a 0.05 significance level.
Similar Pfirrmann grade distributions were found in both patients and controls (Table 2). Also, EP changes were common findings in both patients and controls. Modic changes were more common in patients, while Schmorl’s nodules were slightly more common in controls.Table 2
Distribution of Pfirrmann grades and morphological changes among patients and controls displayed as absolute and relative numbers of incidences per group
| Patients | Controls | |||
|---|---|---|---|---|
| n | % | n | % | |
| Pfirrmann grade | ||||
| 1 | 9 | 8 | 7 | 12 |
| 2 | 60 | 50 | 34 | 57 |
| 3 | 35 | 29 | 14 | 23 |
| 4 | 16 | 13 | 4 | 7 |
| 5 | 1 | 1.7 | ||
| Modic changes | 39 | 14 | 4 | 3 |
| Schmorl’s nodules | 23 | 8 | 17 | 14 |
| EP changes | 110 | 39 | 41 | 34 |
n number of incidences; EP endplate
Functional differences between patients and controls were found in the vertebra (Table 3). For uMRI, the vertebral T2-value was significantly higher in patients, even when adjusted for the presence of Modic changes and Pfirrmann grade. Also, the T2-value was significantly lower in the superior than in the inferior part of the vertebra. This was true both within and between groups. alMRI did not induce any significant changes in the vertebral T2-value neither for patients nor for controls.Table 3
T2-values for patients and controls, and p values within and between groups for uMRI and alMRI, as well as for alMRI-uMRI with correction for Schmorl’s nodules, EP changes, Modic changes and Pfirrmann grade
| Unit | Patients | p value within group | Controls | p value within group | p value between groups |
|---|---|---|---|---|---|
| uMRI | |||||
| Vertebra superior | 100 ± 11 | 87 ± 12 | 0.01 | ||
| Vertebra inferior | 102 ± 10 | 88 ± 13 | 0.03 | ||
| Difference vertebra superior–inferior | < 0.001 | < 0.001 | 0.9 | ||
| Endplate superior | 30 ± 8 | 28 ± 7 | 0.004 | ||
| Endplate inferior | 39 ± 9 | 34 ± 8 | 0.006 | ||
| Difference endplate superior–inferior | < 0.001 | < 0.001 | 0.2 | ||
| alMRI | |||||
| Vertebra superior | 99 ± 10 | 88 ± 11 | 0.02 | ||
| Vertebra inferior | 100 ± 10 | 89 ± 11 | 0.04 | ||
| Difference vertebra superior–inferior | 0.021 | 0.045 | 0.9 | ||
| Endplate superior | 32 ± 7 | 29 ± 8 | 0.09 | ||
| Endplate inferior | 40 ± 9 | 37 ± 10 | 0.17 | ||
| Difference endplate superior–inferior | < 0.001 | < 0.001 | 0.5 | ||
| alMRI-uMRI | |||||
| Vertebra superior | 0.5 (− 8 to 12) | 0.2 (− 6 to 17) | 0.8 | ||
| Vertebra inferior | − 0.7 (− 10 to 10) | − 0.7 (− 15 to 11) | 0.5 | ||
| Endplate superior | 2 (− 12 to 33) | < 0.001 | 0 (− 13 to 67) | 0.2 | 0.87 |
| Endplate inferior | 0 (− 51 to 37) | 0.95 | 2 (− 25 to 25) | 0.1 | 0.18 |
Data given as mean ± SD or as mean (range)
uMRI unloaded MRI; alMRI axial loading of the spine during MRI
T2-mapping revealed functional differences in EPs between patients and controls. For uMRI, significantly higher EP T2-values were found in patients, even when adjusted for the presence of Schmorl’s nodules, EP signal changes and Pfirrmann grade. alMRI induced significant EP T2-changes in patients, but not in controls. Moreover, significantly higher load-induced T2-changes were found in the superior EPs of patients in comparison with controls, even when adjusted for the presence of Schmorl’s nodules, EP signal changes and Pfirrmann grade. For both patients and controls as well as for uMRI and alMRI, the T2-value was significantly lower in superior than in inferior EPs.
The intra- and interobserver ICC for the vertebral T2-value were excellent (0.9–1.0), for the superior EPs fair to good (0.5–0.6) and for the inferior EPs, good to excellent (0.6–0.8).
This study demonstrated differences between LBP patients and controls in EPs and vertebrae measured with T2-mapping. The significantly higher T2-values measured with uMRI in patient EPs and vertebrae and the significantly higher EP T2-values induced with alMRI in patients were found also after corrections for the presence of visible morphological changes in the conventional T1W- and T2W-images. Hence, T2-mapping and alMRI may have the potential to detect early functional differences in EP and vertebrae between groups, not visualized with conventional diagnostic methods. Importantly, the difference in T2-value between groups may indicate that EPs and vertebrae in LBP patients have altered biodynamical characteristics compared to controls. Additionally, present findings support our previous study that displayed load-induced T2-effects in EPs and difference in T2-value between superior and inferior EPs [14]. Hence, alMRI may reveal functional differences in EPs between patients and controls.
In this study, the prevalence of Modic changes was larger in patients with LBP than in controls (14% in patients and 3% in controls), explaining the larger T2-value found in the patient cohort without Modic correction. Higher T2-values can be expected in inflammatory tissues. For example, in IVDs with hernias, higher T2-values have been shown within the posterior regions, reflecting altered biochemistry, such as increased water content due to an inflammatory process [16]. The persistent higher T2-value in the patient group even after Modic correction might be due to an early inflammation process, not visible in conventional MR images due to limitations in diagnostic performance. Hence, T2-mapping may add new functional information about the vertebral tissue that may improve the understanding of inflammatory Modic changes and the influence on LBP.
Bone marrow inflammation is closely associated with oedema, caused by capillary leakage of fluid into the vertebral tissue due to increased intravascular pressure. The increased intravascular pressure can be either hyperaemic, from increased blood flow to the marrow, or congestive, from decreased venous clearance of the marrow tissue. As such, alMRI may have the potential to influence the intravascular pressure, causing fluid redistribution. However, in contrast to our hypothesis that alMRI has the feasibility to reveal such dynamic behaviour, inflammatory Modic type I changes displayed, in conformity with vertebrae without Modic changes, no load-induced effect.
Our results show that patients display higher EP T2-values and that loading induces larger EP T2-changes in patients in comparison with control. Whether inflammation or other EP changes, such as fractures, erosions or calcifications, are the cause remains to be shown. Nevertheless, it should be pointed out that our findings show that EP examination with T2-mapping during conventional unloaded MRI and alMRI displays differences between groups with and without pain. Additionally, our findings indicate that EPs in LBP patients have altered biochemical characteristics in comparison with controls that are not associated with morphological changes visible in conventional images. Signs of inflammation, certainly not visible in conventional images as morphological changes, could be present in the patient EPs leading to differences in the T2-value and in the load-induced change in the T2-value between cohorts, as discussed above.
Besides displaying differences between groups, T2-mapping also had the feasibility to display differences within groups. Significantly higher T2-values were found in inferior compared with superior EPs and vertebrae. The difference in T2-value most likely reflects known structural differences in EP and vertebral composition. It has been shown in vitro and in animal studies that the inferior EP is thicker, is stiffer, resists load better and has different transport kinetics in comparison with superior EPs [17]. Moreover, the difference in tissue composition between EPs at different positions has indirectly been shown in humans as superior EPs being more prone to burst fractures [18]. Biomechanical in vitro studies on vertebrae also support our findings that the composition of the vertebral tissue is not morphologically homogeneous [19]. Posterior regions of the vertebrae have larger bone volume, more connections, reduced trabecular separation and more plate-like isotropic structures than their corresponding anterior regions. Also, significant heterogeneity exists between posterior superior and inferior regions. The regional variation in vertebral morphology suggests that there is likely also some variation in function and, hence, in measured T2-value between different positions.
Present findings constitute ground data for future studies and encourage further investigations of the EP T2-behaviour. The significant difference in T2-value and load-induced T2-change at a group level might represent impaired integrity of abnormal EPs. Also the wide range of load-induced EP changes, seen at an individual level, might reflect differences in the characteristics between individual EPs [20]. As shown by Rajsekaran et al., the fluid transport over the EP depends on the tissue characteristics. Structural EP changes, like fissures or sclerosis, may alter the permeability of the EP, and this can be shown as altered dynamic contrast-enhanced MRI (DCE-MRI) patterns. Difference in transport behaviour between individual EPs may also be revealed with T2-mapping in combination with alMRI, e.g. as an increase or decrease in load-induced T2-value. Hence, future studies are warranted to investigate the pathophysiological mechanisms behind the divergent behaviours seen between individual EPs.
In this study, the segmented ROI was positioned over the EP zone approximately one pixel away from the visible edge of the IVD and vertebra to reduce the influence of adjacent tissues on the EP T2-value. With use of such strategy, the segmentation does not rely on edges in the image for the delineation and this may affect the reproducibility of the T2-value. Nevertheless, the ICC displayed fair agreement between repeated measurements both within and between observers. Moreover, we found that the reproducibility was sufficiently high for determination of statistical significances between groups.
This study demonstrated significantly higher EP and vertebral T2-values in LBP patients in comparison with controls. In addition, alMRI induced significant T2-changes in the superior EPs for patients but not for controls. Importantly, the T2-differences between the groups may indicate that EPs and vertebrae in LBP patients have altered biodynamical characteristics compared to controls and the higher T2-values measured in patients may represent early inflammation or impaired nutritional transport.
The authors acknowledge support from C4I centre, Sahlgrenska University Hospital, Konrad Helfrid Johanssons Foundation, Felix Neubergh Foundation, ALF grant and Innovation Founding, Västra Götaland Region and AFA Insurance Company.
The authors have no conflict of interests to declare.
586_2018_5824_MOESM1_ESM.pptx (144 kb)Supplementary material 1 (PPTX 143 kb)
© The Author(s) 2018
Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.