Insights into treatment and outcome of fracture-related infection: a systematic literature review
Bezstarosti, H., Van Lieshout, E.M.M., Voskamp, L.W. et al.
Arch Orthop Trauma Surg (2019) 139: 61.
https://doi.org/10.1007/s00402-018-3048-0
Abstract
Introduction
Standardized guidelines for treatment of fracture-related infection (FRI) are lacking. Worldwide many treatment protocols are used with variable success rates. Awareness on the need of standardized, evidence-based guidelines has increased in recent years. This systematic literature review gives an overview of available diagnostic criteria, classifications, treatment protocols, and related outcome measurements for surgically treated FRI patients.
Methods
A comprehensive search was performed in all scientific literature since 1990. Studies in English that described surgical patient series for treatment of FRI were included. Data were collected on diagnostic criteria for FRI, classifications used, surgical treatments, follow-up protocols, and overall outcome. A systematic review was performed according to the PRISMA statement. Proportions and weighted means were calculated.
Results
The search yielded 2051 studies. Ninety-three studies were suitable for inclusion, describing 3701 patients (3711 fractures) with complex FRI. The population consisted predominantly of male patients (77%), with the tibia being the most commonly affected bone (64%), and a mean of three previous operations per patient. Forty-three (46%) studies described FRI at one specific location. Only one study (1%) used a standardized definition for infection. A total of nine different classifications were used to guide treatment protocols, of which Cierny and Mader was used most often (36%). Eighteen (19%) studies used a one-stage, 50 (54%) a two-stage, and seven (8%) a three-stage surgical treatment protocol. Ten studies (11%) used mixed protocols. Antibiotic protocols varied widely between studies. A multidisciplinary approach was mentioned in only 12 (13%) studies.
Conclusions
This extensive literature review shows a lack of standardized guidelines with respect to diagnosis and treatment of FRI, which mimics the situation for prosthetic joint infection identified many years ago. Internationally accepted guidelines are urgently required to improve the quality of care for patients suffering from this significant complication.
Fracture-related infection (FRI) is a serious complication related to musculoskeletal trauma. It can have a devastating impact on a patient’s quality of life and has huge socioeconomic consequences [1]. Patients are often not only unable to participate in social activity due to their limited mobility and function. They also encounter higher direct and indirect health care costs. The results from a recent cost analysis showed that the hospital-related health care costs of infected cases are approximately 6.5-times higher than for non-infected cases, which is much higher than data that were previously published [2, 3, 4]. These results stress the importance of standardized prevention and treatment guidelines, with respect to this serious complication.
Since the beginning of the twentieth century the cornerstones of treatment have been extensive and multiple debridements with dead space management and soft tissue coverage [5]. Antibiotic therapy was added as technology progressed. Now almost a 100 years later, a wide variety of strategies is used (e.g., 1 stage, 2 stage, Masquelet, RIA, Ilizarov methods, different types of local antibiotics) without clear scientific background, resulting in a wide spread of clinical results. The rate of FRI remains at 20–30%, with a reported overall treatment failure of 4–11% [6, 7, 8].
The aim of this review was to give an overview of the diagnostic criteria, classifications, surgical and follow-up protocols, and success rates of all FRI treatment series published over the last decades.
Methods
This study was written according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [9].
Literature search strategy
A comprehensive search was performed with the help of a biomedical information specialist in October 2016 and updated on July 1 2017, using Medline, Embase, Web of Science, Cochrane, and Google Scholar. The search strings are recorded in Appendix 1. All studies that described surgical patient series for treatment of FRI were included. Series needed to be greater than five patients and reported in English. Publications before 1990, studies that did not describe FRI patient treatment, and publications reporting non-original data (e.g., reviews or meta-analyses) were excluded. Inclusion consisted of two phases. During the first phase title and abstract were screened for relevance, and full text articles were obtained. When a full text was not available, the corresponding author was contacted once by email. Full text articles were reviewed in the second phase. All references were reviewed by HB and LWV and included after matching the inclusion criteria. Consensus was reached on all references.
Data extraction
After inclusion, data from each study was independently extracted by two authors (HB and LWV). Disagreements were discussed until agreement was reached. Data were collected in five areas. Part one provided general information from all studies (sample size, age, FRI, and location of FRI). Part two offered information on diagnostic criteria for FRI (given definition of FRI, used classification of FRI, and parameters describing the outcome parameters of FRI).
Part Three focused on data from surgical protocols (number of stages in surgical protocol, type of fixation used, and use of a multidisciplinary approach). Part four described the treatment concept (bone defect size, exact treatment protocol, use of bone, skin or muscle graft, and use of local antibiotics). Part five included the follow-up protocol (bony consolidation without infection after the primary surgical study protocol (primary healing), bony consolidation or amputation without infection at the end of study period (total healing), recurrence of FRI, amputation of the affected limb, number of complications, revision surgery, time to bony union and Hospital Length of Stay (HLOS) and patient reported outcomes).
Analysis
Results were pooled for the total population presented in the included studies. Binomial data were pooled using Medcalc (MedCalc Statistical Software version 17.9.7) (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org; 2017). Heterogeneity was quantified with Cochran’s Q test and I2 statistic, a fixed effects model was used when the I2 was < 40%. A random effects model was used for the pooled analysis when the heterogeneity test was ≥ 40%. Pooled estimates are reported with their 95% confidence intervals (CI).
Since for continuous data, most studies only provided a mean but not the standard deviation, a full meta-analysis was not feasible. Instead, continuous data were pooled by calculating the weighted mean using Microsoft Excel. Sample size of the individual studies was used as weighting factor. The pooled mean is reported with the range.
Results
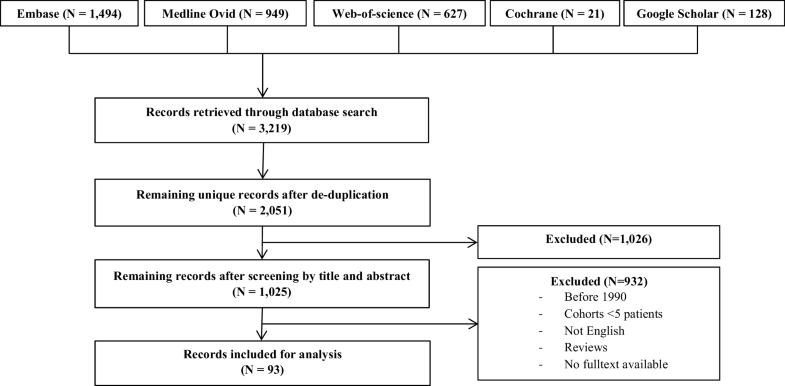
The search identified a total of 2051 unique studies. Figure 1 shows the inclusion flowchart. After selection, 93 studies [8, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101] remained for inclusion, describing 3701 patients with 3711 FRI’s. The population consisted predominantly of male patients (n = 2656; 77%), with a mean age of 42 (range 6–95) years, a mean infection duration of 28 (range 0–154) months and a mean follow-up of 42 (range 6–101) months. Patients had a mean of 3 (range 0–31) operations before study inclusion. Of all studies, 43 described FRI at one specific location. Table 1 shows the reported locations of FRI, with the tibia being the most commonly affected site (n = 2533; 64%), followed by the femur (n = 599; 16%).
Fig. 1Flowchart of the study
Table 1
Overview of locations of FRI
Location of FRI
All studies, N = 3711
Tibia
2533 (68.3%)
Femur
599 (16.1%)
Ankle
124 (3.3%)
Calcaneus
77 (2.1%)
Foot
63 (1.7%)
Humerus
59 (1.6%)
Knee
49 (1.3%)
Fibula
30 (0.8%)
Radius
24 (0.6%)
Forearm
24 (0.6%)
Ulna
18 (0.5%)
Ilium
13 (0.4%)
Elbow
11 (0.3%)
Clavicle
4 (0.1%)
Spine
1 (0.0%)
Skull
1 (0.0%)
Not specified
197 (5.3%)
Lower extremity not defined
41 (1.1%)
Upper extremity not defined
21 (0.6%)
Diagnosis and classification
An overview of all criteria used to diagnose and/or define FRI is given in Table 2. Diagnostic criteria to define FRI were found in 85 (91%) studies. Clinical (n = 83; 89%) and radiological signs (n = 73; 78%) were mostly included in the diagnosis of FRI.Table 2
Overview of parameters used to diagnose or define FRI
Parameters associated with FRI
Number of studies, N = 93
Clinical signs
Purulent drainage (or discharge)
34 (37%)
Dolor (pain)
14 (15%)
Tumor (swelling)
9 (10%)
Calor (warmth)
8 (9%)
Rubor (redness)
7 (8%)
Wound dehiscence/breakdown
7 (8%)
Fever
5 (5%)
Unspecified
46 (49%)
Laboratory testing
C-reactive protein (CRP)
17 (18%)
Unspecified
9 (10%)
Radiological signs
Signs of osteomyelitis
62 (67%)
Evidence of non-union
34 (37%)
Bacteriological/histological findings
Cultures taken
56 (60%)
Unspecified histology
17 (18%)
Unspecified bacteriology
15 (16%)
Other
Time of infection
27 (29%)
No parameters for diagnosis given
8 (9%)
An overview of all described classifications is given in Table 3. A total number of ten different classifications to define infection were found in 47 (51%) studies. The classification of Cierny-Mader was most widely used (N = 34; 37%). The duration of the infection was part of infection classifications in 27 (29%) studies. An overview of all time periods recorded in defining FRI can be found in Table 4. Chronic osteomyelitis was described as an infection-period longer than 6 months in four studies (4%), a period of more than 12 weeks in three studies (3%), a period of more than 6 weeks in three studies (3%), and a period longer than 2 months in two studies (2%). Infected non-union was also classified according to time in 12 studies, of which nine (10%) used 6 months as a cutoff.Table 3
Finally, three studies (3%) subdivided infection into three time periods (acute, subacute and chronic). Of all studies, 66 (71%), did not mention time in the classification of FRI.
Surgical protocols
An overview of surgical protocols is given in Table 5. Surgical treatment protocols differed widely across all studies. Overall, 41 (44%) studies described a FRI located in a single anatomic location, compared with 52 (56%) studies, where multiple locations were described.Table 5
Surgical Protocol and Type of Fixation
Number of stages
Number of studies, N = 93
One-stage
18 (19%)
Two-stage
50 (54%)
Three-stage
7 (8%)
Combination of the above
10 (11%)
Unknown
16 (17%)
Type of fixation
Number of studies, N = 93
Internal
12 (13%)
External
27 (29%)
Bone transport
14 (15%)
Mixed protocols
34 (37%)
Unknown
14 (15%)
A two-stage surgical procedure was used in 50 (54%) studies, followed by a one-stage procedure in 18 (19%), and a three-stage protocol in seven (8%) studies.
Most of the included studies (34; 37%) described a mixture of fracture/bone fixation techniques. Single techniques described were external fixation without bone transport in 27 (29%), followed by external fixation with bone transport in 14 (15%), and internal fixation in twelve (13%). Treatment of bone defects larger than 1 cm were described in 41 (44%) studies.
A multidisciplinary approach in the treatment of FRI was mentioned in 12 (13%) studies, mostly mentioning a team consisting of a trauma or orthopedic surgeon in combination with a plastic surgeon and/or infectious disease (ID) specialist. The different specialties collaborating in such a multidisciplinary team are summarized in Table 6.Table 6
Multidisciplinary approach in treatment of FRI
Specialists involved
Number of studies, N = 12
Trauma/orthopedic surgeon
10 (83%)
Infectious disease specialist
5 (42%)
Plastic surgeon
5 (42%)
Pharmacist
1 (8%)
Radiologist
1 (8%)
Team not defined
3 (25%)
Treatment specifications
An overview of bone grafts used in the treatment of FRI is given in Table 7.
In 62 (67%) studies a total of 1418 bone grafts were described to treat FRI, of which 555 (39%) were cancellous and 381 (27%) were free vascularized bone grafts.Table 7
Bone grafts used in treatment of FRI
Graft type used (62 studies)
N = 1418 (% of total)
Cancellous bone
555 (39)
Iliac crest
445 (31)
RIA (with BMP-7)
76 (5)
Tibia condyle
25 (2)
Femur condyle
9 (1)
Vascularized bone
381 (27)
Vascularized fibula
322 (23)
Latissimus dorsi with rib
41 (3)
Vascularized ilium
18 (1)
Other
27 (2)
Graft not defined
455 (32)
Table 8 summarizes all means by which soft tissue reconstruction was achieved. In 41 (44%) studies a total of 1171 methods to reconstruct soft tissue were described, of which 460 (39%) free flaps, 247 (21%) skin grafts, and 125 (11%) rotational flaps. Local antibiotic therapy was used in 51 (55%) studies. Systemic or oral antibiotic treatment regiments differed widely across studies and will be discussed elsewhere.Table 8
Muscle and skin flaps used in treatment of FRI
Total (41 studies)
N = 1171 (% of total)
Free flap
460 (39)
Latissimus dorsi
206 (18)
Not defined
82 (7)
Gracilis
64 (5)
Rectus abdominis
47 (4)
Scapular skin flap
23 (2)
Serratus anterior
23 (2)
Lateral thigh
15 (1)
Rotational flap
125 (11)
Gastrocnemius
52 (4)
Saphenous
50 (4)
Soleus
23 (2)
Skin
247 (21)
Split skin graft
232 (20)
Full thickness skin graft
15 (1)
Other
76 (1)
Skin/muscle not defined
200 (17)
Follow-up protocols
Details on all parameters used in follow-up of FRI can be found in Table 9.
Routine follow-up episodes were defined in 26 (28%) studies, describing clearly defined appointment protocols in 14 (15%) of them. Follow-up parameters used to identify disease recurrence were based on radiology (N = 49; 53%), serology (N = 32; 34%), and clinical signs (N = 31; 33%).Table 9
Parameters used during follow-up of FRI
Parameter
Number of studies, N = 93
Predefined routine follow-up episodes
26 (28%)
Clinical signs of infection
31 (33%)
Routine radiological check up
49 (53%)
Blood biomarkers
32 (34%)
C-reactive protein
12 (13%)
Erythrocyte sedimentation rate
10 (11%)
Leucocyte count
4 (4%)
Complete blood count
2 (2%)
Undefined
4 (4%)
Bone scoring systems
5 (5%)
ASAMI
4 (4%)
Bahr score
1 (1%)
Functional outcome scoring systems
19 (20%)
Self-defined functionality scores
5 (5%)
Paley’s functionality score
3 (3%)
American orthopaedic foot and ankle society score
1 (1%)
EuroQol 5D
1 (1%)
Johner-Wruhs evaluation criteria
1 (1%)
Lower extremity functionality scale
1 (1%)
Ma’s knee score
1 (1%)
Mazur’s ankle evaluation grading system
1 (1%)
Merchant and Dietz score
1 (1%)
SF-12
1 (1%)
SF-36
1 (1%)
Shahcheraghi and Bayatpoor evaluation score
1 (1%)
Stewart and Hundley criteria
1 (1%)
Two different scoring systems to describe bone quality were found in five (5%) studies. In 19 (20%) studies a functional outcome scoring system was used, describing 13 different functional outcome scores.
Surgical outcome
A summary of surgical outcome is detailed in Table 10. Of all 3711 reported complex FRI cases, bone healing and eradication of infection, without recurrence, was reported in 85% (95% CI 82–88) after the primary surgical study protocol. This percentage increased to 93% (95% CI 91–94) if repeated treatment protocols, including amputations, were taken into account. In 3% (95% CI 3–5) of all cases, amputation was deemed necessary to treat FRI. Recurrence of infection was seen in 9% (95% CI 7–11).Table 10
Outcomes of FRI treatment
Proportional variable
Studies (N)
FRI (N)
Chi2 (pvalue)
I2 value (95% CI)
Pooled proportion (95% CI)
Primary healing
93
3711
*
81% (77–84)
85% (82–88)
Total healing
92
3695
*
77% (72–81)
93% (91–94)
Infection recurrence
89
3598
*
73% (66–78)
9% (7–11)
Amputation rate
83
3226
*
50% (35–61)
3% (3–5)
Continuous variable
Studies (N)
Patients (N)
Weighted meanb
Union time (months)
47
1809
6.63
Surgical revisionsa
58
2110
0.31
Complicationsa
84
3436
0.38
HLOS (months)
14
415
1.39
*p < 0.0001
aPer patient
bSince most of the individual studies did not report a standard deviation (SD) or standard error, no pooled SD could be provided
A total of 0.39 complications per patient were reported, for which 0.31 surgical revisions per patient were needed. Furthermore, bone healing was achieved in a mean of 7 months (2–15), and patients stayed in the hospital for a mean of 1.39 months (0–3).
Discussion
To our knowledge this is the first extensive review showing a complete overview of treatment and outcome of FRI from 1990 until 2017. A literature search has been performed, including 93 articles describing mostly retrospective series of FRI treatment in 3701 patients.
Treatment principles were described by five items. Diagnosis and classification, surgical protocol, treatment concept, follow-up protocol, and outcome, all showed a clear lack of consensus on diagnosis and treatment guidelines for FRI. This mirrors the situation for Prosthetic Joint Infection (PJI), identified many years ago [102].
It seems that basic management concepts of FRI treatment have not altered much since the beginning of the twentieth century [5], resulting in possible suboptimal care for FRI patients. The next section will discuss the discrepancies identified in the five specific domains.
Diagnostic criteria and classification
This study shows that diagnostic criteria to define FRI were mentioned in 91% of all included studies, but no consensus exists on which parameters are relevant. Furthermore, only one study used a standardized definition for FRI (e.g., CDC guidelines) out of 47 studies using a definition. This is in line with conclusions of a previous review of 100 randomized clinical trials aimed at defining FRI [103].
A survey among 2327 orthopedic trauma surgeons in 2017 also confirmed that no consensus exists with respect to which diagnostic criteria should be used to define FRI and almost 90% of the respondents were convinced that a consensus-derived definition of FRI is urgently necessary [104].
Multiple time-related classifications were described in the literature that subdivide FRI into discrete groupings such as acute and chronic infections, or early, delayed and late onset infections [105, 106, 107].
These time windows are, to the best of our knowledge, not based on scientific evidence. This supports the view that they are poorly defined for FRI (e.g., time since injury, or time since onset of symptoms) and somewhat arbitrary (e.g., a 6 week transition from acute to chronic infection [108]). This review confirms that a variety of time windows is used to classify infection and that only 27 (29%) studies reported time in the classification of infection, suggesting that it is not a widely accepted parameter.
The aim of this review was to map all available diagnostic criteria and classifications used when describing patients treated for FRI. Given there are so many different views and no standardized criteria available, an equal comparison is not possible between studies. In the future this can and could be improved if researchers implement the recently developed consensus definition for FRI [108].
Surgical protocols
This systematic review shows an enormous heterogeneity in treatment protocols. In 52 (56%) of all included studies, multiple anatomic locations are mentioned. Furthermore, different treatment strategies are describe (e.g., one-stage, two stage). This means that pooling of data related to outcome of these studies was not possible.
Twelve (13%) of the studies included, made use of a multidisciplinary approach to treat FRI. In these cases, a wide spectrum of team members were described, which also confirms the lack of consensus within this field. Recent literature shows that collaboration between multiple departments is essential to improve the outcome in FRI patients, not only with respect to treatment but also for prevention [109, 110, 111, 112, 113, 114].
Treatment specifications
As discussed before, this review identified many different treatment strategies for different types of FRI. As a consequence, different success rates were published. Due to heterogeneity it is almost impossible to compare outcome between studies. One explanation for this wide variety of published treatment strategies could be the lack of a consensus in the orthopedic trauma community regarding these strategies to manage FRI [103].
Follow-up protocols
Protocolled follow-up of FRI patients was mentioned in 28% of all studies, showing a wide variety of parameters used in monitoring infection and functional outcome. No consensus exists on proper follow-up for this patient population, again emphasizing the need for international consensus. A recent overview confirms the importance of a well-defined follow-up in stratifications of patients [115].
Surgical outcome
Included patients had a mean of three previous operations per patient before inclusion in the identified studies, further emphasizing the difficulty of FRI treatment. However, treatment failure and recurrence of disease rates found in this review occurred in 6–9% of all included cases, leading to amputation of the affected limb in 3–5%, which is a lower percentage than previously published [6, 7, 8]. This could be explained by underreporting of bad outcome, since surgeons tend to publish successful cases more easily than failures. Such publication bias is often seen in retrospective cohort series, which made up the majority of the series.
The patient-related outcome was calculated as a weighted mean of all included studies, including all available treatment options on different locations of FRI and different lengths of bone defects. Therefore, this outcome is in no way specific and it may only be seen as an overview of various patient-related outcomes in current studies.
Limitations
This review was performed using a literature search with respect to FRI, based on terms that existed before a widely used definition of FRI was available. The lack of a definition makes it difficult to compare studies. In March 2018 a consensus definition of FRI from an international expert group has been published [108], finally offering the possibility to standardize reports and improve published literature.
In 66 (71%) of all studies no timescale was reported for infection, limiting the possibility to give a reliable overview of acute/early/delayed-onset FRI.
A better methodological quality in describing patient series is an absolute must, so comparison between series is possible ultimately leading to improvement of treatment.
We need to organize published work in such a way that comparison of either different surgical protocols or different types of FRI treated with the same surgical protocol is possible, further emphasizing the need for a uniform consensus on diagnosis and treatment of FRI.
Most series published do not provide information on individual patients, and do not supply median and standard deviation for any variable needed to perform statistical comparison between studies. To improve comparative analysis of the literature in the future, there is a need for a standard scientific notation of published data, ultimately leading to improvement in treatment strategies.
Conclusion
This extensive literature review shows that the majority of studies report diagnostic criteria for FRI, and half of all studies describe FRI with a definition. There is an enormous heterogeneity of disease variation in and between reported patient series, surgical treatment protocols, and a lack of follow-up reports. This confirms the lack of standardized guidelines with respect to diagnosis and treatment of FRI, and mimics the situation for PJI identified many years ago. Standardized reporting and internationally accepted guidelines are urgently required to improve research and ultimately the quality of care for patients suffering from this significant and sometimes devastating complication.
Notes
Acknowledgements
The authors thank Mr. Wichor M. Bramer, biomedical information specialist (Erasmus MC, University Medical Center Rotterdam, Rotterdam, The Netherlands), for his help in conducting the systematic literature search.
Funding
There is no funding source.
Compliance with ethical standards
Conflict of interest
The authors have no conflicts of interest to disclose.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
Informed consent was not applicable in this study.
Appendix 1: Search terms used for the individual databases
a.Medline OVID: (“osteitis”/ OR “osteomyelitis”/ OR (osteitis OR osteomyelitis).ab,ti.) AND (exp “Fractures, Bone”/ OR (fracture* OR nonunion* OR malunion* OR nonunited* OR malunited* OR posttraum* OR post-traum*).ab,ti.) AND (“Surgical Procedures, Operative”/ OR “debridement”/ OR osteitis/su OR osteomyelitis/su OR (surger* OR surgic* OR debridement*).ab,ti.) AND (“observational study”/ OR exp “Cohort Studies”/ OR “Case-Control Studies”/ OR “Cross-Sectional Studies”/ OR “multicenter study”/ OR “comparative study”/ OR “clinical study”/ OR exp “clinical trial”/ OR “Random Allocation”/ OR exp “treatment outcome”/ OR (((observation* OR comparativ*) ADJ6 (stud* OR data OR research)) OR cohort* OR longitudinal* OR retrospectiv* OR prospectiv* OR ((case OR cases OR match*) ADJ3 control*) OR (cross ADJ section*) OR correlation* OR multicenter* OR multi-center* OR follow-up* OR followup* OR clinical* OR trial OR random* OR (treatment ADJ3 (outcome* OR fail* OR success*))).ab,ti.) NOT (letter OR news OR comment OR editorial OR congresses OR abstracts).pt. AND english.la.
b.Embase: (‘osteitis’/de OR ‘osteomyelitis’/de OR ‘chronic osteomyelitis’/de OR (osteitis OR osteomyelitis):ab,ti) AND (‘fracture’/exp OR ‘posttraumatic complication’/de OR (fracture* OR nonunion* OR malunion* OR nonunited* OR malunited* OR posttraum* OR post-traum*):ab,ti) AND (‘surgery’/de OR ‘surgical technique’/de OR ‘debridement’/de OR ‘osteitis’/exp/dm_su OR (surger* OR surgic* OR debridement*):ab,ti) AND (‘observational study’/exp OR ‘cohort analysis’/exp OR ‘longitudinal study’/exp OR ‘retrospective study’/exp OR ‘prospective study’/exp OR ‘case control study’/de OR ‘cross-sectional study’/de OR ‘correlational study’/de OR ‘major clinical study’/de OR ‘multicenter study’/de OR ‘comparative study’/de OR ‘follow up’/de OR ‘clinical study’/de OR ‘clinical article’/de OR ‘clinical trial’/exp OR ‘randomization’/exp OR ‘intervention study’/de OR ‘open study’/de OR ‘treatment outcome’/exp OR (((observation* OR comparativ*) NEAR/6 (stud* OR data OR research)) OR cohort* OR longitudinal* OR retrospectiv* OR prospectiv* OR ((case OR cases OR match*) NEAR/3 control*) OR (cross NEXT/1 section*) OR correlation* OR multicenter* OR multi-center* OR follow-up* OR followup* OR clinical* OR trial OR random* OR (treatment NEAR/3 (outcome* OR fail* OR success*))):ab,ti) NOT ([Conference Abstract]/lim OR [Letter]/lim OR [Note]/lim OR [Editorial]/lim) AND [english]/lim
c.Web of Science: TS=(((osteitis OR osteomyelitis)) AND ((fracture* OR nonunion* OR malunion* OR nonunited* OR malunited* OR posttraum* OR post-traum*)) AND ((surger* OR surgic* OR debridement*)) AND ((((observation* OR comparativ*) NEAR/5 (stud* OR data OR research)) OR cohort* OR longitudinal* OR retrospectiv* OR prospectiv* OR ((case OR cases OR match*) NEAR/2 control*) OR (cross NEAR/1 section*) OR correlation* OR multicenter* OR multi-center* OR follow-up* OR followup* OR clinical* OR trial OR random* OR (treatment NEAR/2 (outcome* OR fail* OR success*))))) AND DT=(article) AND LA=(english)
d.Cochrane: ((osteitis OR osteomyelitis):ab,ti) AND ((fracture* OR nonunion* OR malunion* OR nonunited* OR malunited* OR posttraum* OR post-traum*):ab,ti) AND ((surger* OR surgic* OR debridement*):ab,ti)
1.Metsemakers WJ, Kuehl R, Moriarty TF, Richards RG, Verhofstad MHJ, Borens O, Kates S, Morgenstern M (2018) Infection after fracture fixation: current surgical and microbiological concepts. Injury 49(3):511–522PubMedCrossRefGoogle Scholar
2.Metsemakers WJ, Smeets B, Nijs S, Hoekstra H (2017) Infection after fracture fixation of the tibia: analysis of healthcare utilization and related costs. Injury 48(6):1204–1210PubMedCrossRefGoogle Scholar
4.Thakore RV, Greenberg SE, Shi H, Foxx AM, Francois EL, Prablek MA, Nwosu SK, Archer KR, Ehrenfeld JM, Obremskey WT, Sethi MK (2015) Surgical site infection in orthopedic trauma: a case-control study evaluating risk factors and cost. J Clin Orthop Trauma 6(4):220–226PubMedCrossRefPubMedCentralGoogle Scholar
5.Whire JR (1919) Chronic Traumatic Osteomyelitis, it’s pathology and treatment. First published. Lewis, Boca RatonGoogle Scholar
6.Kanakaris N, Gudipati S, Tosounidis T, Harwood P, Britten S, Giannoudis PV (2014) The treatment of intramedullary osteomyelitis of the femur and tibia using the Reamer-Irrigator-Aspirator system and antibiotic cement rods. Bone Joint J 96-B(6):783–788PubMedCrossRefGoogle Scholar
7.Huh J, Stinner DJ, Burns TC, Hsu JR, Late Amputation Study T (2011) Infectious complications and soft tissue injury contribute to late amputation after severe lower extremity trauma. J Trauma 71(1 Suppl):S47–S51PubMedCrossRefGoogle Scholar
8.Bose D, Kugan R, Stubbs D, McNally M (2015) Management of infected nonunion of the long bones by a multidisciplinary team. Bone Joint J 97B(6):814–817CrossRefGoogle Scholar
9.Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 151(4):264–269PubMedCrossRefGoogle Scholar
10.Anthony JP, Mathes SJ, Alpert BS (1991) The muscle flap in the treatment of chronic lower-extremity osteomyelitis—results in patients over 5 years after treatment. Plast Reconstr Surg 88(2):311–318PubMedCrossRefGoogle Scholar
11.Aytaç S, Schnetzke M, Swartman B, Herrmann P, Woelfl C, Heppert V, Gruetzner PA, Guehring T (2014) Posttraumatic and postoperative osteomyelitis: surgical revision strategy with persisting fistula. Arch Orthop Trauma Surg 134(2):159–165. https://doi.org/10.1007/s00402-013-1907-2PubMedCrossRefGoogle Scholar
12.Barbarossa V, Matković BR, Vučić N, Bielen M, Gluhinić M (2001) Treatment of osteomyelitis and infected non-union of the femur by a modified Ilizarov technique: follow-up study. Croat Med J 42(6):634–641PubMedGoogle Scholar
14.Caesar BC, Morgan-Jones RL, Warren RE, Wade RH, Roberts PJ, Richardson JB (2009) Closed double-lumen suction irrigation in the management of chronic diaphyseal osteomyelitis: long-term follow-up. J Bone Jt Surg Ser B 91(9):1243–1248. https://doi.org/10.1302/0301-620x.91b9.21768CrossRefGoogle Scholar
15.Calhoun JH, Henry SL, Anger DM, Cobos JA, Mader JT (1993) The treatment of infected nonunions with gentamicin-polymethylmethacrylate antibiotic beads. Clin Orthop Relat Res (295):23–27Google Scholar
16.Campbell R, Berry MG, Deva A, Harris IA (2011) Aggressive management of tibial osteomyelitis shows good functional outcomes. Eplasty 11:e3PubMedPubMedCentralGoogle Scholar
17.Chadayammuri V, Herbert B, Hao J, Mavrogenis A, Quispe JC, Kim JW, Young H, Hake M, Mauffrey C (2017) Factors associated with adverse postoperative outcomes in patients with long bone post-traumatic osteomyelitis. Eur J Orthop Surg Traumatol 27:877. https://doi.org/10.1007/s00590-017-1962-4PubMedCrossRefGoogle Scholar
18.Chan YS, Ueng SWN, Wang CJ, Lee SS, Chao EK, Shin CH (1998) Management of small infected tibial defects with antibiotic-impregnated autogenic cancelleus
bone grafting. J Trauma Inj Infect Crit Care 45(4):758–764. https://doi.org/10.1097/00005373-199810000-00023CrossRefGoogle Scholar
21.Chen CM, Su AW, Chiu FY, Chen TH (2010) A surgical protocol of ankle arthrodesis with combined ilizarov’s distraction-compression osteogenesis and locked nailing for osteomyelitis around the ankle joint. J Trauma Inj Infect Crit Care 69(3):660–665. https://doi.org/10.1097/TA.0b013e3181bc01e6CrossRefGoogle Scholar
22.Chim H, Sontich JK, Kaufman BR (2011) Free tissue transfer with distraction osteogenesis is effective for limb salvage of the infected traumatized lower extremity. Plast Reconstr Surg 127(6):2364–2372PubMedCrossRefGoogle Scholar
24.Cierny Iii G (1999) Infected tibial nonunions (1981–1995). The evolution of change. Clin Orthop Relat Res (360):97–105Google Scholar
25.Conway J, Mansour J, Kotze K, Specht S, Shabtai L (2014) Antibiotic cement-coated rods: an effective treatment for infected long bones and prosthetic joint nonunions. Bone Joint J 96-B(10):1349–1354PubMedCrossRefGoogle Scholar
26.de Souza FI, Zumiotti AV, Mattar R, Wei TH, de Resende MR, Torres LR (2009) Use of gastrocnemius muscle on treatment of infected injuries of the knee. Acta Ortop Bras 17(4):239–241CrossRefGoogle Scholar
27.Dendrinos GK, Konto
s S, Lyritsis E (1995) Use of the Ilizarov technique for treatment of non-union of the tibia associated with infection. J Bone Joint Surg Am 77(6):835–846PubMedCrossRefGoogle Scholar
29.Doi K, Kawakami F, Hiura Y, Oda T, Sakai K, Kawai S (1995) One-stage treatment of infected bone defects of the tibia with skin loss by free vascularized osteocutaneous grafts. Microsurgery 16(10):704–712PubMedCrossRefGoogle Scholar
31.Emami A, Mjoberg B, Larsson S (1995) Infected tibial nonunion. Good results after open cancellous bone grafting in 37 cases. Acta Orthop Scand 66(5):447–451PubMedCrossRefGoogle Scholar
33.Eralp L, Balci HI, Kocaoglu M, Sen C, Celiktas M, Tomak Y, Gulsen M, Dikmen G (2016) Is acute compression and distraction superior to segmental bone transport techniques in chronic tibial osteomyelitis ? Comparison of distraction osteogenesis techniques. Acta Orthop Belg 82(3):599–609PubMedGoogle Scholar
34.Eralp L, Kocaoǧlu M, Polat G, Baş A, Dirican A, Azam ME (2012) A comparison of external fixation alone or combined with intramedullary nailing in the treatment of segmental tibial defects. Acta Orthop Belg 78(5):652–659PubMedGoogle Scholar
35.Eralp L, Kocaoglu M, Rashid H (2007) Reconstruction of segmental bone defects due to chronic osteomyelitis with use of an external fixator and an intramedullary nail: surgical technique. J Bone Jt Surg Ser A 89(SUPPL. 2 PART 2):183–195. https://doi.org/10.2106/jbjs.g.00306CrossRefGoogle Scholar
36.Erdinger K, Windhofer C, Papp C (2001) Osteomuscular latissimus dorsi scapula flap to repair chronic, posttraumatic osteomyelitis of the lower leg. Plastic Reconstr Surg 107:1430–1435CrossRefGoogle Scholar
37.Esterhai JL Jr, Sennett B, Gelb H, Heppenstall RB, Brighton CT, Osterman AL, LaRossa D, Gelman H, Goldstein G (1990) Treatment of chronic osteomyelitis complicating nonunion and segmental defects of the tibia with open cancellous bone graft, posterolateral bone graft, and soft-tissue transfer. J Trauma 30(1):49–54PubMedCrossRefGoogle Scholar
38.Fan CY, Hsieh MS, Chen WM, Chen CF (2011) Successful management of infected intramedullary nailing with reaming, lavage, and insertion of antibiotic-impregnated cement rods. J Exp Clin Med 3(3):137–141. https://doi.org/10.1016/j.jecm.2011.04.002CrossRefGoogle Scholar
39.Ferguson JY, Dudareva M, Riley ND, Stubbs D, Atkins BL, McNally MA (2014) The use of a biodegradable antibiotic-loaded calcium sulphate carrier containing tobramycin for the treatment of chronic osteomyelitis: a series of 195 cases. Bone Jt J 96 B(6):829–836. https://doi.org/10.1302/0301-620x.96b6.32756CrossRefGoogle Scholar
40.Fleiter N, Walter G, Bosebeck H, Vogt S, Buchner H, Hirschberger W, Hoffmann R (2014) Clinical use and safety of a novel gentamicin-releasing resorbable bone graft substitute in the treatment of osteomyelitis/osteitis. Bone Joint Res 3(7):223–229PubMedCrossRefPubMedCentralGoogle Scholar
43.Heppert V, Hochstein P, Aymar M, Wentzensen A (1995) The treatment of infected tibial pilon fractures. Eur J Orthop Surg Traumatol 5(2):161–163PubMedCrossRefGoogle Scholar
44.Humm G, Noor S, Bridgeman P, David M, Bose D (2014) Adjuvant treatment of chronic osteomyelitis of the tibia following exogenous trauma using OSTEOSET-T: a review of 21 patients in a regional trauma centre. Strateg Trauma Limb Reconstr 9(3):157–161CrossRefGoogle Scholar
45.Ibnoulkhatib A, Lacroix J, Moine A, Archambaud M, Bonnet E, Laffosse JM (2012) Post-traumatic bone and/or joint limb infections due to Clostridium spp. Orthop Traumatol Surg Res 98(6):696–705CrossRefGoogle Scholar
46.Isenberg JS, Costigan W (1998) Microvascular transfers in the treatment of massive long-bone osteomyelitis: filling the dugout canoe. J Reconstr Microsurg 14(2):83–87PubMedCrossRefGoogle Scholar
51.Lin CC, Chen CM, Chiu FY, Su YP, Liu CL, Chen TH (2012) Staged protocol for the treatment of chronic tibial shaft osteomyelitis with Ilizarov’s technique followed by the application of intramedullary locked nail. Orthopedics 35(12):e1769–e1774PubMedCrossRefGoogle Scholar
52.Liu T, Yu XD, Zhang XS, Li ZH, Zeng W (2012) One-stage management of post-traumatic tibial infected nonunion using bone transport after debridement. Turk J Med Sci 42(6):1111–1120Google Scholar
55.Marsh JL, Prokuski L, Biermann JS (1994) Chronic infected tibial nonunions with bone loss: conventional techniques versus bone transport. Clin Orthop Relat Res 301:139–146Google Scholar
56.McKee MD, Li-Bland EA, Wild LM, Schemitsch EH (2010) A prospective, randomized clinical trial comparing an antibiotic- impregnated bioabsorbable bone substitute with standard antibiotic-impregnated cement beads in the treatment of chronic osteomyelitis and infected nonunion. J Orthop Trauma 24(8):483–490. https://doi.org/10.1097/BOT.0b013e3181df91d9PubMedCrossRefGoogle Scholar
57.McKee MD, Wild LM, Schemitsch EH, Waddell JP (2002) The use of an antibiotic-impregnated, osteoconductive, bioabsorbable bone substitute in the treatment of infected long bone defects: early results of a prospective trial. J Orthop Trauma 16(9):622–627. https://doi.org/10.1097/00005131-200210000-00002PubMedCrossRefGoogle Scholar
58.Megas P, Saridis A, Kouzelis A, Kallivokas A, Mylonas S, Tyllianakis M (2010) The treatment of infected nonunion of the tibia following intramedullary nailing by the Ilizarov method. Injury 41(3):294–299PubMedCrossRefGoogle Scholar
62.Nenad T, Reiner W, Michael S, Reinhard H, Hans H (2010) Saphenous perforator flap for reconstructive surgery in the lower leg and the foot: a clinical study of 50 patients with posttraumatic osteomyelitis. J Trauma Inj Infect Crit Care 68(5):1200–1207. https://doi.org/10.1097/TA.0b013e3181d03d18CrossRefGoogle Scholar
63.Niikura T, Lee SY, Iwakura T, Sakai Y, Kuroda R, Kurosaka M (2016) Antibiotic-impregnated calcium phosphate cement as part of a comprehensive treatment for patients with established orthopaedic infection. J Ortop Sci 21(4):539–545. https://doi.org/10.1016/j.jos.2016.05.003CrossRefGoogle Scholar
64.Patzakis MJ, Mazur K, Wilkins J, Sherman R, Holtom P (1993) Septopal beads and autogenous bone grafting for bone defects in patients with chronic osteomyelitis. Clin Orthop Relat Res (295):112–118Google Scholar
65.Patzakis MJ, Scilaris TA, Chon J, Holtom P, Sherman R (1995) Results of bone grafting for infected tibial nonunion. Clin Orthop Relat Res (315):192–198Google Scholar
66.Polyzois VD, Galanakos SP, Tsiampa VA, Papakostas ID, Kouris NK, Avram AM, Papalois AE, Ignatiadis IA (2011) The use of Papineau technique for the treatment of diabetic and non-diabetic lower extremity pseudoarthrosis and chronic osteomyelitis. Diabetic Foot Ankle 2:1–7. https://doi.org/10.3402/dfa.v2i0.5920CrossRefGoogle Scholar
67.Prasarn ML, Ahn J, Achor T, Matuszewski P, Lorich DG, Helfet DL (2009) Management of infected femoral nonunions with a single-staged protocol utilizing internal fixation. Injury 40(11):1220–1225PubMedCrossRefGoogle Scholar
68.Prasarn ML, Ouellette EA, Miller DR (2010) Infected nonunions of diaphyseal fractures of the forearm. Arch Orthop Trauma Surg 130(7):867–873PubMedCrossRefGoogle Scholar
69.Qiang Z, Jun PZ, Jie XJ, Hang L, Bing LJ, Cai LF (2007) Use of antibiotic cement rod to treat intramedullary infection after nailing: preliminary study in 19 patients. Arch Orthop Trauma Surg 127(10):945–951PubMedCrossRefGoogle Scholar
71.Reichert P, Rutowski R, Gosk J, Zimmer K, Wiacek R (2007) Treatment of infected nonunion of long bones. Adv Clin Exp Med 16(3):403–409Google Scholar
72.Sadek AF, Laklok MA, Fouly EH, Elshafie M (2016) Two stage reconstruction versus bone transport in management of resistant infected tibial diaphyseal nonunion with a gap. Arch Orthop Trauma Surg 136(9):1233–1241PubMedCrossRefGoogle Scholar
73.Sancineto CF, Barla JD (2008) Treatment of long bone osteomyelitis with a mechanically stable intramedullar antibiotic dispenser: nineteen consecutive cases with a minimum of 12 months follow-up. J Trauma Inj Infect Crit Care 65(6):1416–1420. https://doi.org/10.1097/TA.0b013e31818c6a09CrossRefGoogle Scholar
74.Scholz AO, Gehrmann S, Glombitza M, Kaufmann RA, Bostelmann R, Flohe S, Windolf J (2015) Reconstruction of septic diaphyseal bone defects with the induced membrane technique. Injury 46(Suppl 4):S121–S124PubMedCrossRefGoogle Scholar
75.Schröter S, Ateschrang A, Flesch I, Stöckle U, Freude T (2015) First mid-term results after cancellous allograft vitalized with autologous bone marrow for infected femoral non-union. Wien Klin Wochenschr 128(21–22):827–836. https://doi.org/10.1007/s00508-015-0797-4PubMedCrossRefGoogle Scholar
76.Selhi HS, Mahindra P, Yamin M, Jain D, De Long WG Jr, Singh J (2012) Outcome in patients with an infected nonunion of the long bones treated with a reinforced antibiotic bone cement rod. J Orthop Trauma 26(3):184–188PubMedCrossRefGoogle Scholar
78.Shen L, Dong Y, Zhang C, Guo Q, Shou D, Zhang Y, Zhang Z, Wong KKL, Ghista DN, Huang W (2015) Chronic osteomyelitis treatment: a clinical and pharmaco-kinetic study of vancomycin impregnated calcium sulphate. J Med Imaging Health Inf 5(1):36–42. https://doi.org/10.1166/jmihi.2015.1362CrossRefGoogle Scholar
79.Shyam AK, Sancheti PK, Patel SK, Rocha S, Pradhan C, Patil A (2009) Use of antibiotic cement-impregnated intramedullary nail in treatment of infected non-union of long bones. Indian J Orthop 43(4):396–402PubMedCrossRefPubMedCentralGoogle Scholar
80.Ueng SW, Wei FC, Shih CH. (1999) Management of femoral diaphyseal infected nonunion with antibiotic beads local therapy, external skeletal fixation, and staged bone grafting. J Trauma Inj Infect Crit Care 46(1):97–103. https://doi.org/10.1097/00005373-199901000-00016CrossRefGoogle Scholar
81.Tajsi N, Winkel R, Hoffmann R, Husum H (2009) Sural perforator flap for reconstructive surgery in the lower leg and the foot: a clinical study of 86 patients with post-traumatic osteomyelitis. J Plast Reconstr Aesth Surg 62(12):1701–1708. https://doi.org/10.1016/j.bjps.2008.06.091CrossRefGoogle Scholar
82.Tan Y, Wang X, Li H, Zheng Q, Li J, Feng G, Pan ZJ (2011) The clinical efficacy of the vacuum-assisted closure therapy in the management of adult osteomyelitis. Arch Orthop Trauma Surg 131(2):255–259PubMedCrossRefGoogle Scholar
83.Thonse R, Conway J (2007) Antibiotic cement-coated interlocking nail for the treatment of infected nonunions and segmental bone defects. J Orthop Trauma 21(4):258–268PubMedCrossRefGoogle Scholar
84.Tong K, Zhong Z, Peng Y, Lin C, Cao S, Yang Y, Wang G (2017) Masquelet technique versus Ilizarov bone transport for reconstruction of lower extremity bone defects following posttraumatic osteomyelitis. Injury 48(7):1616–1622. https://doi.org/10.1016/j.injury.2017.03.042PubMedCrossRefGoogle Scholar
86.Tulner SAF, Schaap GR, Strackee SD, Besselaar PP, Luitse JSK, Marti RK (2004) Long-term results of multiple-stage treatment for posttraumatic osteomyelitis of the Tibia. J Trauma Inj Infect Crit Care 56(3):633–642CrossRefGoogle Scholar
87.Ueng WN, Shih CH (1995) Management of infected tibial intramedullary nailing using an organized treatment protocol. Eur J Orthop Surg Traumatol 5(2):151–155PubMedCrossRefGoogle Scholar
88.Vitkus K, Vitkus M, Cierny Iii G, Nahai F (1992) Reconstruction of large infected tibia defects. Ann Plast Surg 29(2):97–108PubMedCrossRefGoogle Scholar
90.Wasko MK, Borens O (2013) Antibiotic cement nail for the treatment of posttraumatic intramedullary infections of the tibia: midterm results in 10 cases. Injury 44(8):1057–1060PubMedCrossRefGoogle Scholar
91.Wu CC (2011) Single-stage surgical treatment of infected nonunion of the distal Tibia. J Orthop Trauma 25(3):156–161PubMedCrossRefGoogle Scholar
92.Wu CH, Yuan LJ, Chan YS, Chen ACY, Lee MS, Ueng SWN (2007) Conditions affecting treatment of pertrochanteric osteomyelitis. Chang Gung Med J 30(5):414–422PubMedGoogle Scholar
93.Xu K, Fu X, Li YM, Wang CG, Li ZJ (2014) A treatment for large defects of the tibia caused by infected nonunion: Ilizarov method with bone segment extension. Ir J Med Sci 183(3):423–428PubMedCrossRefGoogle Scholar
94.Xu XY, Zhu Y, Liu JH (2009) Treatment of calcaneal osteo
myelitis with free serratus anterior muscle flap transfer. Foot Ankle Int 30(11):1088–1093PubMedCrossRefGoogle Scholar
95.Yang C, Geng S, Fu C, Sun J, Bi Z (2013) A minimally invasive modified reverse sural adipofascial flap for treating posttraumatic distal tibial and calcaneal osteomyelitis. Int J Lower Extrem Wounds 12(4):279–285. https://doi.org/10.1177/1534734613511637CrossRefGoogle Scholar
96.Yang YF, Xu ZH, Zhang GM, Wang JW, Hu SW, Hou ZQ, Xu DC (2013) Modified classification and single-stage microsurgical repair of posttraumatic infected massive bone defects in lower extremities. J Reconstr Microsurg 29(9):593–600. https://doi.org/10.1055/s-0033-1348064PubMedCrossRefGoogle Scholar
97.Yin P, Zhang LH, Li TT, Zhang LC, Wang GQ, Li JT, Liu JH, Zhou JF, Zhang Q, Tang PF (2015) Infected nonunion of tibia and femur treated by bone transport. J Orthop Surg Res 10:49PubMedCrossRefPubMedCentralGoogle Scholar
98.Zalavras CG, Patzakis MJ, Thordarson DB, Shah S, Sherman R, Holtom P (2004) Infected fractures of the distal tibial metaphysis and plafond—achievement of limb salvage with free muscle flaps, bone grafting, and ankle fusion. Clin Orthop Relat Res 427:57–62CrossRefGoogle Scholar
101.Zych GA, Hutson JJ Jr (1995) Diagnosis and management of infection after tibial intramedullary nailing. Clin Orthop Relat Res (315):153–162Google Scholar
102.Cats-Baril W, Gehrke T, Huff K, Kendoff D, Maltenfort M, Parvizi J (2013) International consensus on periprosthetic joint infection: description of the consensus process. Clin Orthop Relat Res 471(12):4065–4075PubMedCrossRefPubMedCentralGoogle Scholar
103.Metsemakers WJ, Kortram K, Morgenstern M, Moriarty TF, Meex I, Kuehl R, Nijs S, Richards RG, Raschke M, Borens O, Kates SL, Zalavras C, Giannoudis PV, Verhofstad MHJ (2018) Definition of infection after fracture fixation: a systematic review of randomized controlled trials to evaluate current practice. Injury 49(3):497–504PubMedCrossRefGoogle Scholar
104.Morgenstern M, Moriarty TF, Kuehl R, Richards RG, McNally MA, Verhofstad MHJ, Borens O, Zalavras C, Raschke M, Kates SL, Metsemakers WJ (2018) International survey among orthopaedic trauma surgeons: lack of a definition of fracture-related infection. Injury 49(3):491–496PubMedCrossRefGoogle Scholar
105.Borens O, Helmy N (2016) [Infected osteosynthesis]Infizierte Osteosynthese. Chirurg 87(10):822–830PubMedCrossRefGoogle Scholar
106.Willenegger H, Roth B (1986) [Treatment tactics and late results in early infection following osteosynthesis] Behandlungstaktik und Spatergebnisse bei Fruhinfekt nach Osteosynthese. Unfallchirurgie 12(5):241–246PubMedCrossRefGoogle Scholar
107.Kleber C, Schaser KD, Trampuz A (2015) [Complication management of infected osteosynthesis: therapy algorithm for peri-implant infections] Komplikationsmanagement bei infizierter Osteosynthese: therapiealgorithmus bei periimplantaren Infektionen. Chirurg 86(10):925–934PubMedCrossRefGoogle Scholar
108.Metsemakers WJ, Morgenstern M, McNally MA, Moriarty TF, McFadyen I, Scarborough M, Athanasou NA, Ochsner PE, Kuehl R, Raschke M, Borens O, Xie Z, Velkes S, Hungerer S, Kates SL, Zalavras C, Giannoudis PV, Richards RG, Verhofstad MHJ (2018) Fracture-related infection: a consensus on definition from an international expert group. Injury 49(3):505–510PubMedCrossRefGoogle Scholar
109.Greene LR (2012) Guide to the elimination of orthopedic surgery surgical site infections: an executive summary of the Association for Professionals in Infection Control and Epidemiology elimination guide. Am J Infect Control 40(4):384–386PubMedCrossRefGoogle Scholar
111.Dudareva M, Ferguson J, Riley N, Stubbs D, Atkins B, McNally M (2017) Osteomyelitis of the pelvic bones: a multidisciplinary approach to treatment. J Bone Jt Infect 2(4):184–193PubMedCrossRefPubMedCentralGoogle Scholar
112.Bose D, Kugan R, Stubbs D, McNally M (2015) Management of infected nonunion of the long bones by a multidisciplinary team. Bone Joint J 97-B(6):814–817PubMedCrossRefGoogle Scholar
113.Kortram K, Bezstarosti H, Metsemakers WJ, Raschke MJ, Van Lieshout EMM, Verhofstad MHJ (2017) Risk factors for infectious complications after open fractures; a systematic review and meta-analysis. Int Orthop 41(10):1965–1982PubMedCrossRefGoogle Scholar
114.Metsemakers WJ, Onsea J, Neutjens E, Steffens E, Schuermans A, McNally M, Nijs S (2017) Prevention of fracture-related infection: a multidisciplinary care package. Int Orthop 41(12):2457–2469PubMedCrossRefGoogle Scholar
115.Obremskey WT, Higgins TF, Bettger JP, Vrahas MS, Lundy DW (2018) Use of patient-related outcomes after orthopaedic trauma: helpful or not so much? J Orthop Trauma 32(Suppl 1):S48–S51PubMedCrossRefGoogle Scholar
Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article
CrossMarkCite this article as:Bezstarosti, H., Van Lieshout, E.M.M., Voskamp, L.W. et al. Arch Orthop Trauma Surg (2019) 139: 61. https://doi.org/10.1007/s00402-018-3048-0