Classification of coronal imbalance in adult scoliosis and spine deformity: a treatment-oriented guideline
Obeid, I., Berjano, P., Lamartina, C. et al. Eur Spine J (2019) 28: 94. https://doi.org/10.1007/s00586-018-5826-3
Abstract
Introduction
In adult spinal deformity (ASD), sagittal imbalance and sagittal malalignment have been extensively described in the literature during the past decade, whereas coronal imbalance and coronal malalignment (CM) have been given little attention. CM can cause severe impairment in adult scoliosis and ASD patients, as compensatory mechanisms are limited. The aim of this paper is to develop a comprehensive classification of coronal spinopelvic malalignment and to suggest a treatment algorithm for this condition.
Methods
This is an expert’s opinion consensus based on a retrospective review of CM cases where different patterns of CM were identified, in addition to treatment modifiers. After the identification of the subgroups for each category, surgical planning for each subgroup could be specified.
Results
Two main CM patterns were defined: concave CM (type 1) and convex CM (type 2), and the following modifiers were identified as potentially influencing the choice of surgical strategy: stiffness of the main coronal curve, coronal mobility of the lumbosacral junction and degeneration of the lumbosacral junction. A surgical algorithm was proposed to deal with each situation combining the different patterns and their modifiers.
Conclusion
Coronal malalignment is a frequent condition, usually associated to sagittal malalignment, but it is often misunderstood. Its classification should help the spine surgeon to better understand the full spinal alignment of ASD patients. In concave CM, the correction should be obtained at the apex of the main curve. In convex CM, the correction should be obtained at the lumbosacral junction.
Graphical abstract
These slides can be retrieved under Electronic Supplementary Material.
Coronal malalignment (CM) is defined as lateral deviation of the T1 plumbline with substantial displacement from the midline of the pelvis for more than 20 mm. CM has also been referred to in the literature as coronal imbalance [1, 2, 3], but balance is obviously a dynamic concept, and our spinal assessment is done on full spine X-rays that are static and not dynamic examinations; therefore, balance or imbalance should rather be called alignment or malalignment. CM is evaluated in standing position in ambulatory patients and in sitting position in patients who are not able to walk, and it has been well documented and analyzed in patients with cerebral palsy [4, 5]. In this clinical situation, CM (originating from spinal deformity) causes pelvic obliquity which leads to gait disturbances in patients who are able to walk, and to asymmetric ischial compression in sitting position and difficulties to maintain proper sitting position in patients who are not able to walk. Pelvic obliquity can also lead to costo-iliac conflict and costal pain.
In patients suffering from adult spine deformity (ASD), CM has been rarely described and the literature provides little guidance for surgical indications [6, 7]. Nevertheless, CM (or coronal trunk inclination CTI) is regularly seen in patients with ASD who have undergone or not undergone surgery.
Patients suffering from CM do not have many compensatory mechanisms available for this specific condition. The only natural compensatory mechanism is contralateral knee and hip flexion, which is extremely uncomfortable for the patient. In addition, unlike the sagittal malalignment (SM), which disappears in sitting position, coronal malalignment is present in sitting and standing position and is irrelevant only with the patient laying down horizontal.
Consequences of CM on patient’s satisfaction are not neglectable, especially when it appears or worsens after the surgery. CM is rarely isolated and it is frequently associated to sagittal plane deformities and SM [8].
Surgical correction of sagittal and coronal malalignment needs biplanar maneuvers, which may be challenging and may need different kinds of osteotomies [9, 10].
The aim of this paper is to develop a comprehensive classification of coronal spinopelvic malalignment and to suggest a treatment algorithm for this condition.
Materials and methods
Type of study Expert’s opinion consensus and case studies.
Methods A collection of cases with a variety of CM scenarios was restrospectively obtained from the authors’ centers surgical files. Cases representing categories of CM patterns were selected. The relevant factors (treatment modifiers) influencing surgical planning and execution and their effect on surgical outcomes in terms of alignment were defined.
Subsequently, categories of CM and modifiers were listed. Finally for each pattern and relevant factors, the most appropriate indications for planning and surgical execution were assigned.
Curve flexibility was assessed by supine bending films in the majority of cases unless the lumbosacral curve was stiff, in that case fulcrum-bending test (with bolster) in lateral position with horizontal beam were performed. A specific concern was to evaluate L4 endplate obliquity on bending films. The flexibility of the curve should be modulated by the possibility of obtaining some interbody mobility by posterior or anterior release. This will cause some rigid curves to potentially become flexible and that may avoid performing three-column osteotomy (3-CO). To evaluate sagittal plane flexibility, bolster extension lateral film was obtained. In addition, MRI and CT scans were systematically performed to evaluate the degeneration of the lumbosacral junction as well as the canal caliber.
Results
CM patterns
Two main CM patterns were identified.
Concave CM (Type 1) is defined as CM with coronal T1 plumbline falling at the side of the concavity of the main coronal curve (Fig. 1).Open image in new windowFig. 1Type 1 This case is an example of concave CM: the coronal T1 plumb line falls in the concave side of the main coronal curve. The simulated correction of the main curve shows its global effect, resulting in correction of the coronal malalignment
Convex CM (Type 2) is defined as CM with coronal T1 plumbline falling at the side of the convexity of the main coronal curve (Fig. 2).Open image in new windowFig. 2Type 2 Example of convex CM: the coronal T1 plumb line falls in the convex side of the main coronal curve. The simulated correction of the main curve shows its global effect, resulting in increase in the coronal malalignment
The relevance of these patterns depends on the different effects that correction of the main coronal curve has on each pattern. In the case of concave CM, correction of the main curve is coupled with reduction in CM. Conversely, correction of the main curve in convex CM results in increase in CM.
Treatment modifiers
The following modifiers were identified as potentially influencing the choice of surgical strategy:
Stiffness of the main coronal curve:
Flexible
Rigid or fused
Coronal mobility of the lumbosacral (LS) junction
Mobile
Rigid
Degeneration of the lumbosacral junction
Absent or mild
Moderate or advanced (Table 1)Table 1Treatment-oriented classification of coronal malalignmentMain typesSubtypesMain featuresCorrective maneuversType 1Concave CM Coronal malalignment toward the concavity of the main curve Type 1AMain L/TL curveMain curve with apex between T12 and L4 Type 1A1Flexible main L/TLMain curve is flexible on bending or potentially after posterior releaseCorrection of the main curve with posterior release and instrumentation is usually sufficient to correct both main curve and CM. Multilevel PCO and/or anterior support might be necessary to provide correction in the sagittal plane Type 1A2Rigid main L/TLMain curve is very rigid or fused3-CO at the apex of the main curve and instrumentation provides correction of both main curve and CM. SM can be simultaneously fixed by biplanar correction at the 3-CO level Type 1BMain thoracic curveMain curve with apex above T123-CO usually needed for coronal or coronal and sagittal correctionType 2Convex CM Coronal malalignment toward the convexity of the main curve Type 2AMain L/TL curveMain curve with apex between T12 and L4 Type 2A1Normal LS junctionL4–S1 not degenerated and coronally mobileAggressive correction of the main curve with lower instrumented vertebra at L4 or above. Expect patient’s self-balancing over time Type 2A2Rigid/degenerated LS junctionL4–S1 degenerated or stiffCorrection and instrumentation of main lumbar curve with extension to pelvis. 3-CO or aggressive release of the LS junction Type 2BMain LS curveMain curve with apex below L4aShort correction of the LS junction with 3-CO at the apex of the LS curve (usually L5, occasionally L4 or S1)aThis is a convex-like CM as it is apparently a convex CM in respect to the L curve, yet in theory, it should be a concave CM in respect to the LS curve (main curve in this case)
Combination of patterns and modifiers and classification
1.Type 1: Concave coronal malalignmentIn concave CM, the correction of the main curve improves the CM, thus we can talk about convergent corrective objectives. The ability to correct the CM depends on the correctability of the main curve. The need of three-column osteotomies in order to obtain correction of CM depends on the location and flexibility of the main curve.
1.a.Type 1A: Main lumbar/thoracolumbar curveThe correction strategy will depend on the flexibility of the main curve.
1.a.1.Type 1A1: Flexible L/TL main curveIf the main curve is flexible or potentially flexible, posterior release and instrumented correction allows at the same time the correction of the scoliotic curve and the CM. SM is generally present in association with CM. Simultaneous correction in both planes is necessary. If the major curve is flexible, posterior column osteotomies [11] are usually sufficient to correct the curve, which improves and corrects the CM. The sagittal plane is usually addressed efficiently by the same actions (Figs. 3, 4, 5).Open image in new windowFig. 3Type 1A1 A 48-year-old woman suffering from a severe spinal deformity. Global kyphosis leads to a large compensation at the hip and knee levels. Despite major pelvic retroversion and knee flexion, patient is still anteriorly imbalanced. The trunk is also shifted to the right (concave) side. Lateral bending films showed good flexibility of the main curveOpen image in new windowFig. 4Type 1A1 Posterior column osteotomies allow a good correction of the sagittal plane, of the lumbar scoliotic curve and (as a consequence of main curve correction in concave CM) of the coronal malalignmentOpen image in new windowFig. 5Type 1A1 The same strategy shown in Figs. 3 and 4 in a 78-year-old woman
1.a.2.Type 1A2: Rigid L/TL main curveWhen the main curve is rigid, 3-CO may be indicated. The location of the 3-CO should be determined according to the direction of the coronal correction needed. The scoliotic deformity changes the shape and the orientation of the vertebrae especially close to the apex of the curve. The vertebra is rotated in the direction of the convexity and deformed with a convex side larger than the concave side. Any 3-CO close to the apex will induce automatically an asymmetric correction with coronal translation in the direction of the convex side. This is helpful in case of concave CM, but can be very harmful in the case of convex CM. The 3-CO performed close to the apex allows sagittal plane correction, scoliosis Cobb angle correction and CM correction at the same time. The use of domino connectors in the convex side of the main curve permits a very effective and safe construct-to-construct compression. It also allows an asymmetric closure of the osteotomy and a biplanar correction (Figs. 6, 7). Details on how to calculate the size of the osteotomy for biplanar correction have been published previously [2].Open image in new windowFig. 6Type 1A2 Severe lumbar kyphoscoliosis associated to a concave coronal malalignment. The stiffness of the curve and the magnitude of the sagittal deformity need three-column osteotomy to achieve satisfactory correction. The choice of the apical vertebra is essential in this case: the surgeon takes benefit from the vertebral asymmetry to perform asymmetrical bone resection and correction. Sagittal plane correction allows a better sagittal alignment without the need of any compensatory mechanismOpen image in new windowFig. 7Type 1A2 The use of a domino connector allows a construct-to-construct compression and an asymmetric osteotomy closure and correction. The coronal plane correction is achieved and maintained at follow-up. You can notice in the AP view indirect signs of sagittal plane correction (the inclination of the innominate line of the pelvis is changed as a consequence of normalization of pelvic tilt)
1.b.Type 1B: Concave CM with main thoracic or cervicothoracic curve.As previously discussed, in the majority of patients with concave CM, the major curve is located in the lumbar spine but in some cases the CM is at the side of the concavity of a thoracic or cervicothoracic curve. In these situations, a three-column osteotomy is often needed because of the stiffness and the magnitude of the major thoracic curve [10, 12]. An experimented team may perform these techniques safely. When both coronal and sagittal deformities are present, 3-CO can be shaped to correct simultaneously both planes (Figs. 8, 9).Open image in new windowFig. 8Type 1B A 67-year-old patient, multiple previous spinal fusion and osteotomy surgeries. She is suffering from major sagittal and coronal malalignment. The CM is on the concave side of the main thoracic curve. A posterior vertebral column resection is performed at the apex of the thoracic curve to correct the major curve and the coronal and sagittal malalignment at the same time. Notice the disappearance of knee flexion after surgeryOpen image in new windowFig. 9Type 1B A 58-year-old man with neglected post-traumatic deformity; the head of the patient is tilted toward the concavity of the cervicothoracic curve. This coronal deformity was also associated to a post-traumatic kyphosis. An asymmetric T5 PSO allows a correction in both planes. One domino connector is placed on convex side permitting the correction in both planes by asymmetric compression
2.Type 2: Convex coronal malalignmentConvex CM is defined by a deviation of the trunk on the convex side of the main coronal curve, which usually is a lumbar (apex below L1 and above L4), thoracolumbar (apex at T12 or L1) or
lumbosacral main curve (apex at or below L4). The correction of the lumbar curve will increase the CM by creating a straight spine based on an oblique takeoff, and we talk about divergent corrective objectives. Many specific subtypes can be identified; all of them have in common an oblique takeoff at the lumbosacral junction. The correction of convex CM depends on the correction of the lumbosacral curve. The primary curve may be lumbar or thoracolumbar (more frequent situation) with compensatory lumbosacral fractional curve, but sometimes (congenital, iatrogenic, post-traumatic and rarely degenerative) it can be lumbosacral with compensatory lumbar curve. The correction strategy will depend on many factors including the driver of the deformity, which should always be fused, but also the degeneration and stiffness of the compensatory curve which can lead to more extended fusion. The need of three-column osteotomies depends mainly on the stiffness of the lumbosacral curve.
2.a.Type 2A: Main lumbar or thoracolumbar curveWhen surgery is indicated, the correction of the main curve will increase the coronal malalignment. The correction strategy will depend on the characteristics of the lumbosacral segment.
2.a.1.Type 2A1: Flexible and non-degenerated lumbosacral junctionIf the lumbosacral junction is not degenerate and flexible, after correction of the main lumbar or thoracolumbar curve an indirect correction of the lumbosacral compensatory curve can be achieved by patient’s self-balancing after correction. It can be called active coronal realignment. In order to achieve this self-balancing, two conditions should be present in addition to the previous ones (no major degeneration, flexible LS junction). The first condition is to have at least two mobile segments below the fusion, which means that the distal fused level should be L4 or above. This is important in order to have enough mobility to correct L4 obliquity. The second condition is to obtain enough correction of the main curve to horizontalize the distal end vertebra (Fig. 10). This is the ideal situation in order to spare the lumbosacral junction from fusion. Distal fusion limit should be at L4 or above and the correction of the main curve should be maximized. In such cases, worsening of CM may be observed in the immediate postoperative period but it will improve during follow-up. The phenomenon of active realignment of the lumbosacral junction is probably related to biomechanical muscular improvement after the main curve correction. It needs many weeks to be completed because of many reasons: the muscular weakness after surgery, extraspinal soft tissue tension (fascia, iliolumbar ligaments) and disk retraction in the concave side of the lumbosacral curve. Rehabilitation and corrective short lumbosacral brace may sometimes help during the initial postoperative period.Open image in new windowFig. 10Type 2A1 A 62-year-old woman, suffering from L3 and L4 left nerve root compression associated to lumbar curve progression and L3–L4 laterolisthesis. Coronal imbalance is on the convex side; the lumbosacral junction presents only mild degeneration. At 6 weeks after a posterior T11L4 instrumented fusion, CM increased. At 12 months, spontaneous correction of the CM and a horizontal L4–L5 disk is appreciated, which is maintained 8 years postoperatively. Active realignment (by the patient muscle action) provided progressive and stable correction of the non-fused lumbosacral curve
2.a.2.Type 2A2: Degenerated, stiff or operated lumbosacral junctionIf the lumbosacral junction needs to be fused because of its degeneration, stiffness or need of extensive root decompression, the surgeon must achieve complete coronal plane correction during the surgery. There is no possibility of spontaneous correction after the surgery in case of fusion to L5 or below. In convex CM, fusion to L5 should be avoided, because it does not allow enough correction of CM during surgery and patient’s active realignment is unlikely to happen after surgery. Sacral fixation with iliac extension is necessary to correct the obliquity with a solid lever arm on the sacropelvic foundation. If the lumbosacral curve is degenerated but still flexible, coronal realignment of the LS junction can be obtained by mobilizing the interbody spaces and generous posterior release. This can be achieved by anterior or posterior approaches including interbody release and cages (Figs. 11, 12, 13, 14). Conversely, when the lumbosacral area is rigid, the correction of the lumbosacral curve may need three-column osteotomy and it should be performed at the apex of the lumbosacral (mainly L5 and sometimes L4) curve and not at the apex of the lumbar curve, due to the convex direction of the CM. This information is essential; any osteotomy close to the apex of the lumbar curve will deviate automatically the trunk to the convexity of it and will increase the convex CM. Osteotomy closure with domino connectors allows an asymmetric compression and biplanar correction. The connector should be placed on the side opposite to the CM (Figs. 15, 16). In other words, the correction should be performed from the concave side of the lumbar curve (side opposite to the CM) whatever is the technique used.Open image in new windowFig. 11Type 2A2 A 78-year-old patient suffering from low back pain with major disability and reduced walking distance. She also presented painful left iliocostal conflict due to her major CM and SM. This is a convex CM with degenerated and kyphotic lumbosacral junction. Correction films showed flexible lumbosacral deformity in both planes. Lateral bending films were taken to evaluate coronal plane flexibility; posterior extension bolster film with horizontal beam was taken to evaluate sagittal plane flexibility. The position of the bolster is very important to improve its predictive accuracyOpen image in new windowFig. 12Type 2A2 (same case of Fig. 11). In this case of convex CM, the correction strategy was as follows: posterior and interbody release by transforaminal approach of the lumbosacral curve forms its concavity (left side); insertion of asymmetric TLIF cages on the left side and then correction by translation from the right side: concave side, side opposite to the malalignmentOpen image in new windowFig. 13Type 2A2 (same case of Figs. 11, 12). The correction is maintained at 2 yearsOpen image in new windowFig. 14Type 2A2 The same strategy used in a fourth revision surgery with convex CM. See the coronal orientation of the superior end plate of L3 before and after the correction and the asymmetric L3–L4 and L5–S1 TLIF cages (short black arrows). The correction of the lumbosacral curve needs to exceed in magnitude the correction of the lumbar main curve in order to correct CMOpen image in new windowFig. 15Type 2A2 A 62-year-old women suffering from low back pain and reduced walking autonomy, presented with sagittal and convex coronal malalignment. She had had T11–L5 fusion for lumbar scoliosis 7 years before. On the right, a simulation of correction with a three-column osteotomy performed at the apex of the lumbar curve (L2): with 3-CO at this location CM would be increasedOpen image in new windowFig. 16Type 2A2 Result after L4 asymmetric PSO. The correction of the lumbosacral curve allowed a correction of the convex CM. The domino connector is located at the concave side of the main curve (the opposite side to the CM) to permit an asymmetric osteotomy closure and biplanar correction (coronal and sagittal)
2.b.Type 2B: Main short lumbosacral deformity (convex-like CM)In some cases, the main curve is located at the lumbosacral junction, mainly iatrogenic but also congenital or post-traumatic. As the main curve is lumbosacral, and the T1 plumbline is falling at the side of the concavity of this main curve, therefore, it is theoretically a concave CM but the compensatory lumbar/thoracolumbar curve, that is more obvious to see on the coronal X-ray, suggests that it is a convex CM as the T1 plumbline is falling at the side of its convexity; therefore, this pattern is called convex-like CM. In this situation, the lumbar/thoracolumbar curve may be flexible and not structural and short fusion of the LS curve may be sufficient. Spontaneous correction of the lumbar/thoracolumbar curve is expected after lumbosacral curve correction. This pattern of deformity needs often three-column osteotomy at L5 level [13]. As previously mentioned, the main curve is lumbosacral, so strictly speaking, the direction of CM would be concave (in respect to the LS curve); therefore, the general rule (that applies on concave CM cases) of performing an osteotomy at the apex of the main curve (L5 in most cases) would be appropriate (Figs. 17, 18, 19, 20).Open image in new windowFig. 17Type 2B Short iatrogenic lumbosacral curve in a 58-year-old patient operated six times at the lumbosacral junction. In this case, the CM is located at the convex side of the lumbar curve which is compensatory and flexible, but the main coronal deformity is actually located at the lumbosacral junction, this is a convex-like CMOpen image in new windowFig. 18Type 2B As a case of convex-like CM, the rule for concave coronal malalignment applied, an asymmetric 3-CO was performed at the apex of the main deformity (in this case at the apex of the lumbosacral junction): The L5 asymmetric PSO provided a correction of the lower lumbar lordosis and at the same time of the coronal malalignment. Notice that the closure of the osteotomy was done from the right side through a domino connector and that multiple rod technique was usedOpen image in new windowFig. 19Type 2B A 17-year-old girl, presented with congenital lumbosacral scoliosis and coronal malalignment. In this case again the main and most stiff deformity is located in the lumbosacral area. The lumbar curve was flexible and compensatory. This is a case of convex-like CM (the coronal malalignment is at the concave side of the main curve, the lumbosacral one, but at the convex side of the obviously seen compensatory lumbar curve)Open image in new windowFig. 20Type 2B In this case (same as Fig. 19) of convex-like CM with rigid main curve, a 3-CO at the apex of the main coronal curve was indicated (PSO of the hemivertebra S1) with L4-pelvic fusion. The result was maintained at 8-year follow-up
3.Type 0: Coronally aligned spineHow to avoid postoperative coronal malalignment in a preoperatively aligned spineSevere lumbar scoliotic curves are frequently associated to a stiff lumbosacral compensatory curve. The correction of the main curve is usually easier to obtain than the lumbosacral one and this may lead to substantial correction in the lumbar curve and more partial correction of the LS curve, resulting in an oblique takeoff of the lumbar spine, a mismatch between the two curves (L and LS) and finally CM toward the convexity of the lumbar curve. Therefore, a type 0 may potentially become a type 2 after surgical correction. To avoid postoperative CM, the surgeon should realize a balanced correction of both curves. That can be achieved by a controlled correction avoiding overcorrection of the lumbar curve and an aggressive, wide release and correction of the lumbosacral curve (Fig. 21).Open image in new windowFig. 21Type 0 A 68-year-old woman presented with a major kyphoscoliotic lumbar curve. Combined posterior correction and anterior interbody fusion was performed. Harmonious correction of the lumbar and lumbosacral curves permitted to avoid postoperative coronal malalignment
Discussion
CM can be the consequence of extraspinal disease such as hip or knee contractures, lower limb length discrepancy, severe deformity of the lower limbs, deformity of the pelvis or neurological conditions such as Parkinson’s disease or Pisa syndrome [14]. Extraspinal causes of CM are out of the scope of this article. More generally, CM is usually (but not always) associated to scoliotic deformity of the lumbar spine, and SM is frequently seen in association with CM.
In recent years, ASD has received substantial attention by clinicians and researchers, but most of this attention has focused on various aspects of sagittal alignment. One possible explanation is the fact that while some early research showed associations between both CM and SM with health-related quality of life (HRQoL) [15], other influential studies did not find substantial correlation of CM with HRQoL [16]. In this scenario, correction of SM has received substantial attention in the literature [17], and rules for very precise calculation of the amount of correction needed in the sagittal plane are widely available [18, 19].
In spite of this little attention in the literature, CM may cause severe impairment of the function, alteration of self-image and pain due to costo-iliac conflict, and it is the experience of the authors that moderate grades of CM are poorly tolerated by many patients, especially in the presence of a fused spine or in association with SM.
Moreover, surgery for ASD frequently fails to correct CM or even worsens it. Bao et al. [3] have found that patients with preoperative convex CM are at higher risk of postoperative persistence or worsening of CM. Ploumis et al. [20] in a retrospective analysis of 54 patients followed-up for 2–5 years after long fusions for ASD found that while sagittal malalignment was consistently reduced by surgery, the prevalence of CM did not change from the preoperative to the early postoperative period. In nearly 60% of the cases, preoperative CM was not corrected by surgery, and nearly 9% of patients without preoperative CM showed new onset of CM early postoperatively. Moreover, additional 18% of patients without early postoperative CM developed new CM during follow-up. Postoperative convex coronal malalignment has been described after fusions with the lowest instrumented vertebra (LIV) at L5 for lumbar scoliosis with the use of transpsoas lateral cages, and the likely mechanism is overcorrection of the main lumbar curve over a stiff L5–S1 segment that cannot correct spontaneously to achieve a horizontal takeoff [21]. The clinical importance of these phenomena has been shown by Koller et al. [22], who in a retrospective study on 448 patients found that postoperative CM was associated to worse postoperative clinical outcomes in patients undergoing surgery for ASD.
We hypothesize that the difficulties to correct CM or to maintain coronal alignment when performing surgery for ASD is due to the lack in the literature of clear rules on how to manage or avoid CM. The study of Bao et al. [3] shows the importance of distinguishing convex from concave CM. This separation between concave and convex CM is essential because of its treatment consequences. The correction of the main curve improves concave CM but worsens convex CM as it has been shown in the examples. Surgeons focusing on correcting the main lumbar curve without paying attention to the pattern of CM and the difference in stiffness between the L/TL and the fractional LS curve can actually induce postoperative CM. In this article, we provide guidelines that help the clinician to identify the key factors (patterns and modifiers) and effective strategies of prevention and correction of CM.
Classifications allow us to identify patterns or categories with different causes, behaviors, needs or prognosis. In the field of ASD, different classifications have been described and they provide different types of information. An early classification of ASD by Aebi [23] informed only on the causes of the deformity. Schwab et al. [24] proposed a new classification with metric validation. Though the latter provided information on the impact of the deformity on HRQoL, neither of these classifications provided guidance to treatment.
In 2014, two treatment-oriented classification systems were proposed. The first is by Berjano, aimed to provide guidance to the selection of fusion levels and techniques in adult patients with degenerated or degenerative lumbar deformities [25]. The second is by Lamartina, provided a comprehensive, validated anatomical classification of sagittal deformities, which contained specific suggestions regarding the site of correction and extension of the instrumentation [26]. The current classification of CM comes in the “treatment-oriented flavor” too, as a guide to assist clinicians to obtain better clinical outcomes.
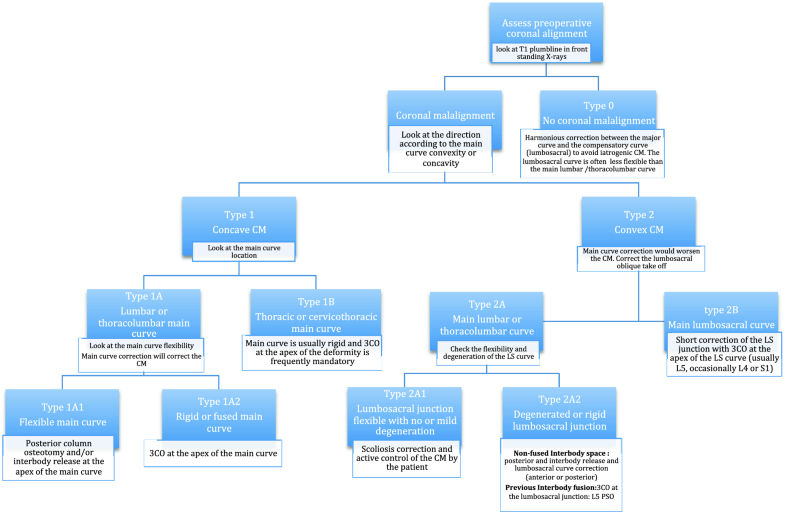
The main weakness of this study is its non-experimental design. Experimental studies have provided some useful insight into the phenomenon of CM. As an example, Bao et al. [27] have shown that postoperative coronal imbalance can improve spontaneously and that lower instrumented vertebra at L4 or higher is correlated to a higher chance of spontaneous correction, which is in agreement with our suggestions. Yet, the complexity of the problem, associated to the multiple variations found (in this classification scheme, we have identified at least six different combinations of patterns and modifiers), makes it virtually impossible to provide a treatment-oriented system based only on experimental data. This article summarizes substantial expertise from the authors, which subsequently will be validated as a whole system in a future paper.A simplified algorithm for management and prevention of CM is provided in Fig. 22.
Fig. 22A proposed algorithm to manage coronal malalignment
Conclusion
Coronal malalignment is a frequent situation, both in non-operated ASD patients and as a new onset deformity in patients operated for ASD that is often misunderstood. It is usually associated to SM. The direction of the coronal malalignment should be described in relation to the main curve of the deformity. In concave coronal malalignment (Type 1), the correction should be obtained at the apex of the main curve; the need of 3-CO depends on its flexibility. In convex and convex-like coronal malalignment (Type 2), the correction should be obtained at the lumbosacral junction. In coronally aligned spine (type 0), to avoid postoperative new onset of CM, hypercorrection of the main lumbar curve should be avoided.
Notes
Compliance with ethical standards
Conflict of interest
The authors declare that they have no conflict of interest.
8.Lamartina C, Berjano P, Petruzzi M, Sinigaglia A, Casero G, Cecchinato R, Damilano M, Bassani R (2012) Criteria to restore the sagittal balance in deformity and degenerative spondylolisthesis. Eur Spine J 21(Suppl 1):S27–S31. https://doi.org/10.1007/s00586-012-2236-9CrossRefGoogle Scholar
13.Alzakri A, Boissiere L, Cawley DT, Bourghli A, Pointillart V, Gille O, Vital JM, Obeid I (2018) L5 pedicle subtraction osteotomy: indication, surgical technique and specificities. Eur Spine J 27:644–651. https://doi.org/10.1007/s00586-017-5403-1CrossRefGoogle Scholar
14.Bourghli A, Guerin P, Vital JM, Aurouer N, Luc S, Gille O, Pointillart V, Obeid I (2012) Posterior spinal fusion from T2 to the sacrum for the management of major deformities in patients with Parkinson disease: a retrospective review with analysis of complications. J Spinal Disord Tech 25:E53–E60. https://doi.org/10.1097/BSD.0b013e3182496670CrossRefGoogle Scholar
15.Glassman SD, Berven S, Bridwell K, Horton W, Dimar JR (2005) Correlation of radiographic parameters and clinical symptoms in adult scoliosis. Spine (Phila Pa 1976) 30:682–688CrossRefGoogle Scholar
16.Lafage V, Schwab F, Skalli W, Hawkinson N, Gagey PM, Ondra S, Farcy JP (2008) Standing balance and sagittal plane spinal deformity: analysis of spinopelvic and gravity line parameters. Spine (Phila Pa 1976) 33:1572–1578. https://doi.org/10.1097/brs.0b013e31817886a2CrossRefGoogle Scholar
17.Obeid I, Boissiere L, Yilgor C, Larrieu D, Pellise F, Alanay A, Acaroglu E, Perez-Grueso FJ, Kleinstuck F, Vital JM, Bourghli A, European Spine Study Group E (2016) Global tilt: a single parameter incorporating spinal and pelvic sagittal parameters and least affected by patient positioning. Eur Spine J 25:3644–3649. https://doi.org/10.1007/s00586-016-4649-3CrossRefGoogle Scholar
18.Berjano P, Cecchinato R, Damilano M, Morselli C, Sansone V, Lamartina C (2013) Preoperative calculation of the necessary correc
tion in sagittal imbalance surgery: validation of three predictive methods. Eur Spine J 22(Suppl 6):S847–S852. https://doi.org/10.1007/s00586-013-3025-9CrossRefGoogle Scholar
19.Berjano P, Langella F, Ismael MF, Damilano M, Scopetta S, Lamartina C (2014) Successful correction of sagittal imbalance can be calculated on the basis of pelvic incidence and age. Eur Spine J 23(Suppl 6):587–596. https://doi.org/10.1007/s00586-014-3556-8CrossRefGoogle Scholar
20.Ploumis A, Simpson AK, Cha TD, Herzog JP, Wood KB (2015) Coronal spinal balance in adult spine deformity patients with long spinal fusions: a minimum 2- to 5-year follow-up study. J Spinal Disord Tech 28:341–347. https://doi.org/10.1097/BSD.0b013e3182aab2ffCrossRefGoogle Scholar
22.Koller H, Pfanz C, Meier O, Hitzl W, Mayer M, Bullmann V, Schulte TL (2016) Factors influencing radiographic and clinical outcomes in adult scoliosis surgery: a study of 448 European patients. Eur Spine J 25:532–548. https://doi.org/10.1007/s00586-015-3898-xCrossRefGoogle Scholar
27.Bao H, He S, Liu Z, Zhu Z, Qiu Y, Zhu F (2015) Will immediate postoperative imbalance improve in patients with thoracolumbar/lumbar degenerative kyphoscoliosis? A comparison between Smith-Petersen osteotomy and pedicle subtraction osteotomy with an average 4 years of follow-up. Spine (Phila Pa 1976) 40:E293–E300. https://doi.org/10.1097/brs.0000000000000744CrossRefGoogle Scholar
Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.